

Summary
Risk of cardiovascular disease\in patients with rheumatoid arthritis persisted at similar rates at 3- and 10-year follow-ups, despite the increased use of statins, antihypertensive agents, and tumor necrosis factor-blocking agents, according to a 10-year prospective study. This article presents data from the Cardiovacular Research and Rheumatoid Arthritis study [CARRÉ; Van Halm VP et al. Ann Rheum Dis 2009].
- Rheumatology Clinical Trials
- Rheumatoid Arthritis
- Rheumatology Clinical Trials
- Rheumatology
- Rheumatoid Arthritis
Risk of cardiovascular disease (CVD) in patients with rheumatoid arthritis (RA) persisted at similar rates at 3- and 10-year follow-ups, despite the increased use of statins, antihypertensive agents, and tumor necrosis factor-blocking agents, according to a 10-year prospective study. Alper M. van Sijl, MD, VU University Medical Center, Amsterdam, The Netherlands, presented data from the Cardiovacular Research and Rheumatoid Arthritis study [CARRÉ; Van Halm VP et al. Ann Rheum Dis 2009]. The CARRÉ investigators compared changes in CV risk factors, RA-related factors, and anti-inflammatory and cardioprotective medication use in RA patients who did or did not develop CVD over 10 years, starting in 2000 to 2001.
RA is associated with a 2-fold increased risk of CVD and up to a 2-fold increase in mortality [Peters MJL et al. Arthritis Rheum 2009]. The increased risk may be attributable to a patient's CV risk profile, chronic inflammation, or undertreatment [Solomon DH et al. Ann Rheum Dis 2010]. Most previous research accounts only for CV- and RA-related associations at baseline [del Rincón ID et al. Arthritis Rheum 2001].
The 353 study participants had a mean age of 63 years and 34% were men. Median disease duration was 7 years. Medication use at baseline was biologicals by only 1% of participants, methotrexate 60%, prednisone 17%, nonsteroidal anti-inflammatory drugs 69%, statins only 12%, and antihypertensives only 26%. The baseline incidence of CVD was 16.1%, the mean RA disease activity score at 28 joints (DAS28) was 3.91±1.36, and the health assessment questionnaire score was 0.75 (0.25 to 1.13).
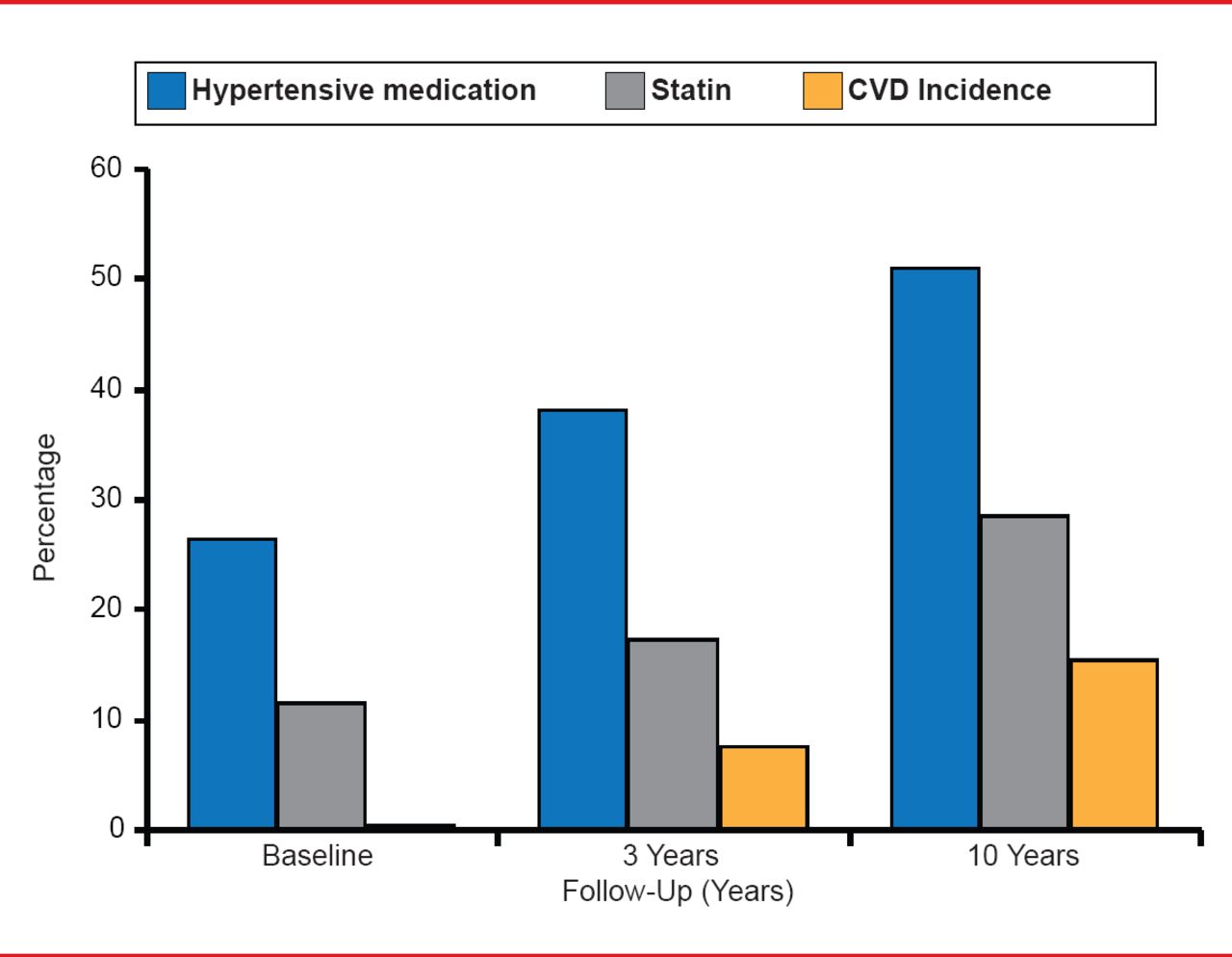
The first follow-up was conducted in 2004 to 2005 and the second in 2010 to 2011. The incidence of CVD and events did not change substantially at Years 3 and 10 (Figure 1), while the use of statins and antihypertensives increased substantially at those time points.

Incidence of CVD and CV Events
Reproduced with permission from AM van Sijl, MD.
In women, baseline systolic blood pressure, the use of antihypertensive drugs, and the estimated renal function were significantly associated with developing CVD (Table 1). No association between RA-related factors and the development of CVD was found in women.
RA-Related and CV-Related Factors Associated With CVD Incidence
The erythrocyte sedimentation rate, an RA-related factor, increased in patients who developed CVD, while there was little change in those without CVD. A similar pattern was seen for the DAS28, which declined initially, but increased in patients who developed CVD. The use of biologicals was substantially increased in patients free of CVD.
Generalized estimating equations evaluated whether changes in RA-related factors or CV-related factors are associated with the incidence of CVD. The CV risk factors played a role in developing CVD at baseline. However, the change in DAS28 was significantly and more strongly associated with developing CVD (HR, 2.03; 95% CI, 1.33 to 3.09) than the traditional CV-related factors in women (Table 2). When adjusting for the use of biologicals, this association was completely negated, which may point out a protective role for biologicals, said Prof. van Sijl.
The Effect of RA- and CV-Related Factors on CVD in Women
The changes in the RA-related factors during follow-up were associated with increased risk of CVD. The presenters concluded that there is a strong indication that improving disease activity and inflammatory markers may positively influence the CV risk in patients with RA.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.