

Summary
Treatment strategies for ST-segment elevation myocardial infarction (STEMI) utilize both pharmacological therapies and devices designed to restore coronary blood flow. While these therapies are generally effective, a proportion of patients with STEMI will develop cardiogenic shock, one of the leading causes of inhospital death post MI. Despite an optimal pharmacomechanical approach, revascularization, and hemodynamic support, the mortality in patients with STEMI complicated by cardiogenic shock remains high.
- Interventional Techniques & Devices
- Myocardial Infarction
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
- Myocardial Infarction
Treatment strategies for ST-segment elevation myocardial infarction (STEMI) utilize both pharmacological therapies and devices designed to restore coronary blood flow. While these therapies are generally effective, a proportion of patients with STEMI will develop cardiogenic shock, one of the leading causes of inhospital death post MI. Despite an optimal pharmacomechanical approach, revascularization, and hemodynamic support, the mortality in patients with STEMI complicated by cardiogenic shock remains high, said Hany Eteiba, MD, University of Glasgow, Glasgow, Scotland.
Prof. Eteiba reviewed effective and active circulatory support strategies that can be used in patients with cardiogenic shock. Extracorporeal membrane oxygenation (ECMO) and left ventricular assist device (LVAD) are two of these approaches and Prof. Eteiba discussed how these devices can be utilized in clinical practice.
Hemodynamic support for patients with acute myocardial infarction complicated by shock can be provided through a variety of available devices (intraaortic ballon pump, Impella, Tandem Heart, etc) that work to increase cardiac output.
Circulatory support can also be provided by ECMO or a LVAD. ECMO is performed by obtaining venous and arterial access and does not require a sternotomy. ECMO can serve as a bridge to recovery, bridge to another hemodynamic support device (total artificial heart or LVAD), or transplantation. The evidence supporting the use of ECMO and the survival rates are shown in Table 1.
Summary of Evidence for Extracorporeal Membrane Oxygenation and Survival Rates after Cardiogenic Shock
The TandemHeart Pump is another circulatory support device utilized in the treatment of patients with cardiogenic shock. In two randomized, controlled trials, TandemHeart, when compared with IABP, improved some hemodynamics measurements. Treatment with TandemHeart did not reduce mortality and complications were increased.
The HeartMate II Long-Term LVAD is implanted surgically and is used as either a destination device or as a bridge to either recovery or transplantation. The HeartMate II is a rotary continuous-flow device that works in parallel with the native left ventricle. It has a percutaneous driveline, a fixed-speed operating mode, and is powered electrically. Some patients treated with a HeartMate II are able to be discharged home after implantation.
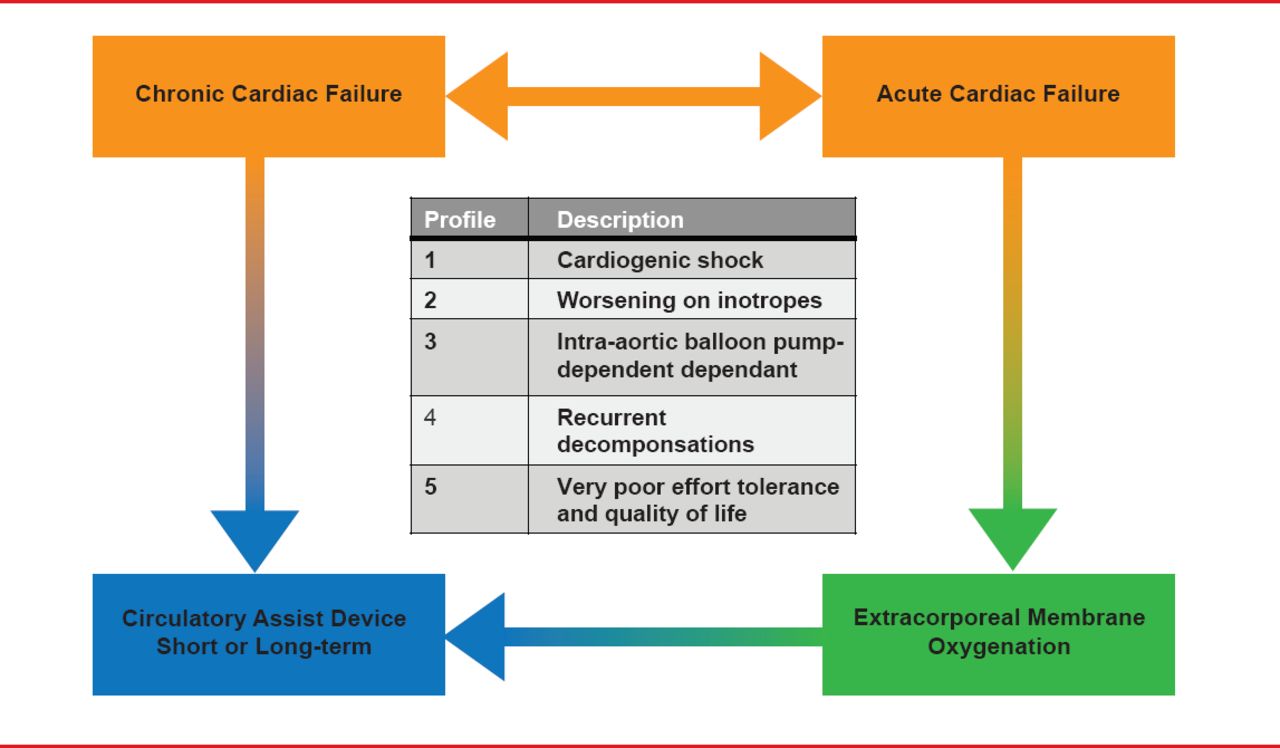
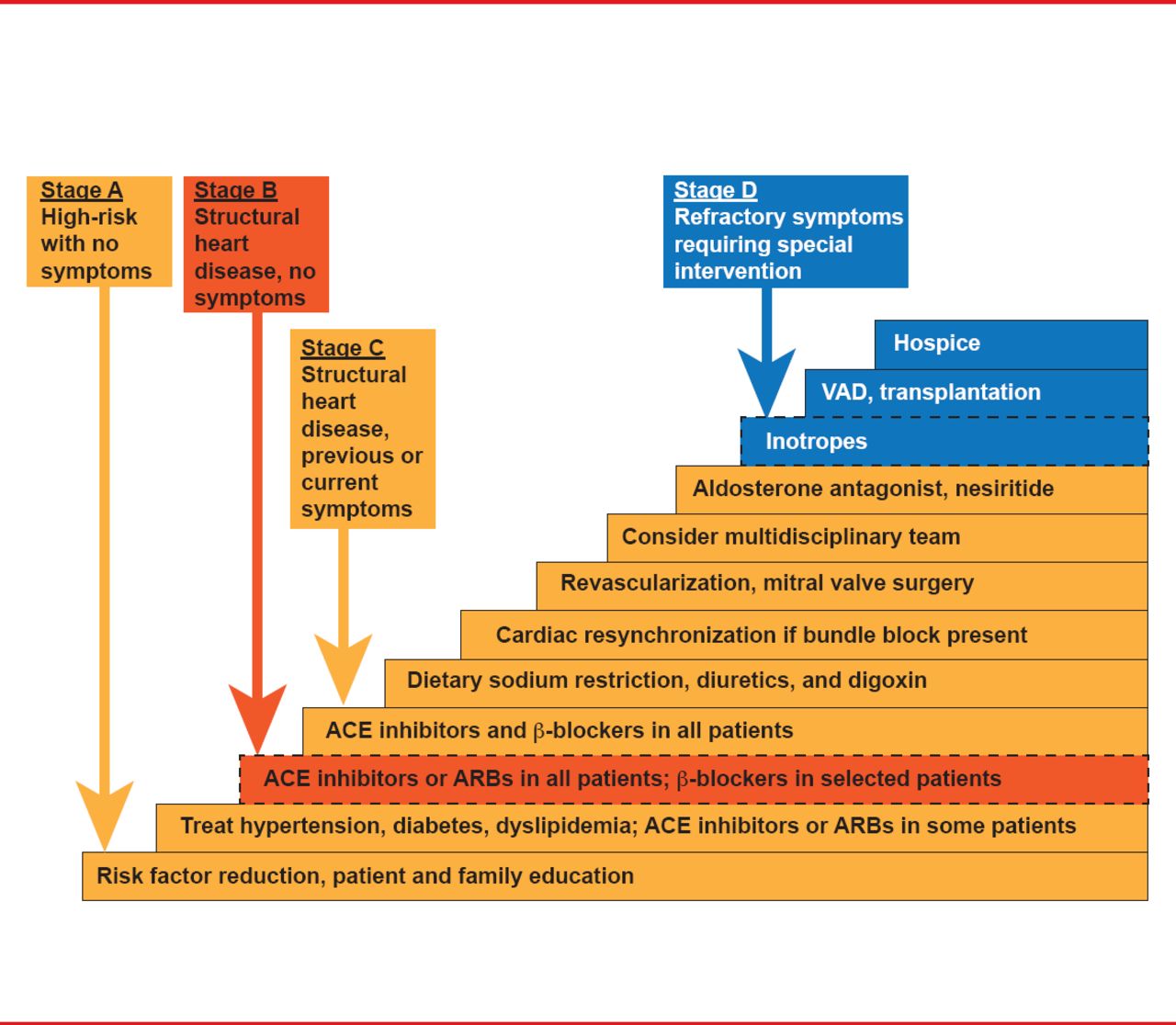
A treatment algorithm for the management of patients with cardiac failure after an MI is shown in Figure 1. Prof. Eteiba reviewed the evolution of cardiac failure in this patient population and treatment recommendations as the disease progresses (Figure 2).

Management of Patients With Cardiac Failure Post Myocardial Infarction
Reproduced with permission from H Etieba, MD.

Treatment Schema for Progressive Cardiac Failure Post-Myocardial Infarction
Reproduced with permission from H Etieba, MD.
The incidence of cardiogenic shock for patients with with STEMI continues to decrease as revascularization rates increase and medical therapy has improved. For example, the TRITON TIMI-38 study [Wiviott SD et al. Lancet 2008] compared the oral antiplatelet prasugrel with clopidogrel. The overall trial showed a reduction in cardiovascular death, MI, and stroke with prasugrel. In addition, treatment with prasugrel reduced stent thrombosis, both early (through Day 30, 0.42% of patients with prasugrel compared with 1.44% of patients with clopidogrel, 71% relative risk reduction [RRR]), and late (Day 31 to Day 450, 0.42% compared with 0.91% of patients, 54% RRR).
The incidence of cardiogenic shock is greater among patients with multivessel coronary artery disease; yet, the optimal revascularization strategy for patients with STEMI and multivessel coronary artery disease remains undefined. The 2005 Practice Guideline from the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions, state that PCI should not be performed in a noninfarct artery during primary PCI in patients without hemodynamic compromise. The current guidelines do note that PCI of a noninfarct-related artery could be considered for patients if the lesion “appeared to be flow limiting in patients with hemodynamic instability”. The 2012 Practice Guidelines from the European Society of Cardiology state that performing PCI in nonculprit vessels is discouraged because of a “gap of evidence.” Numerous observational studies have been published which have found differing results; however, randomized trials are required for this question to be answered in a definitive manner.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.