

Summary
This article reviews the scope of the impact of tobacco on cardiovascular disease (CVD) and its mode of action, the lack of awareness of physicians about smoking cessation tactics, and smoking cessation as a treatment for CVD.
- Smoking Cessation
- Prevention & Screening
- Cardiology & Cardiovascular Medicine
- Smoking Cessation
- Prevention & Screening
The scope of the impact of tobacco on cardiovascular disease (CVD) and its mode of action, the lack of awareness of physicians about smoking cessation tactics, and smoking cessation as a treatment for CVD were reviewed by Georges A. Saade, MD, Bellevue Medical Center, Beirut, Lebanon.
Tobacco use is a risk factor for 6 of the 8 leading causes of death worldwide and is associated with nearly 6 million deaths per year (Figure 1). The use of tobacco is associated with increased CV risk and the use of tobacco is projected to be associated with 175 million deaths worldwide by the year 2030. Given the adverse effects of tobacco utilization, at its 2012 summit on Noncommunicable Diseases, the United Nations endorsed efforts to reduce tobacco abuse in an attempt to reduce premature mortality from CVD.
Cigarette smokers die ∼10 years earlier than nonsmokers and at least half of chronic smokers will die of a tobacco-related disease, according to the British Male Doctors' Study [Doll R et al. BMJ 2004]. Smokers of waterpipes, practiced in Egypt and other countries, are also at risk for developing dependence and other adverse health-related conditions associated with smoking [Maziak W. Addict Behav 2011], contrary to popular opinion that waterpipes are safe. Newer interventions to help smokers quite offer the potential for reducing the smoking rates in the near future. An anonymous survey of 326 cardiologists in Spain revealed that 3 in 4 always ask their patients about smoking and recommend that they quit; 1 in 5 had cessation print materials in their office; and 2 in 5 checked patient progress. However, 73% were unfamiliar with cessation medications and 71% wanted to improve their tobacco treatment skills. [Dalmau R. Heart wire http://www.theheart.org/article/1531389.do].

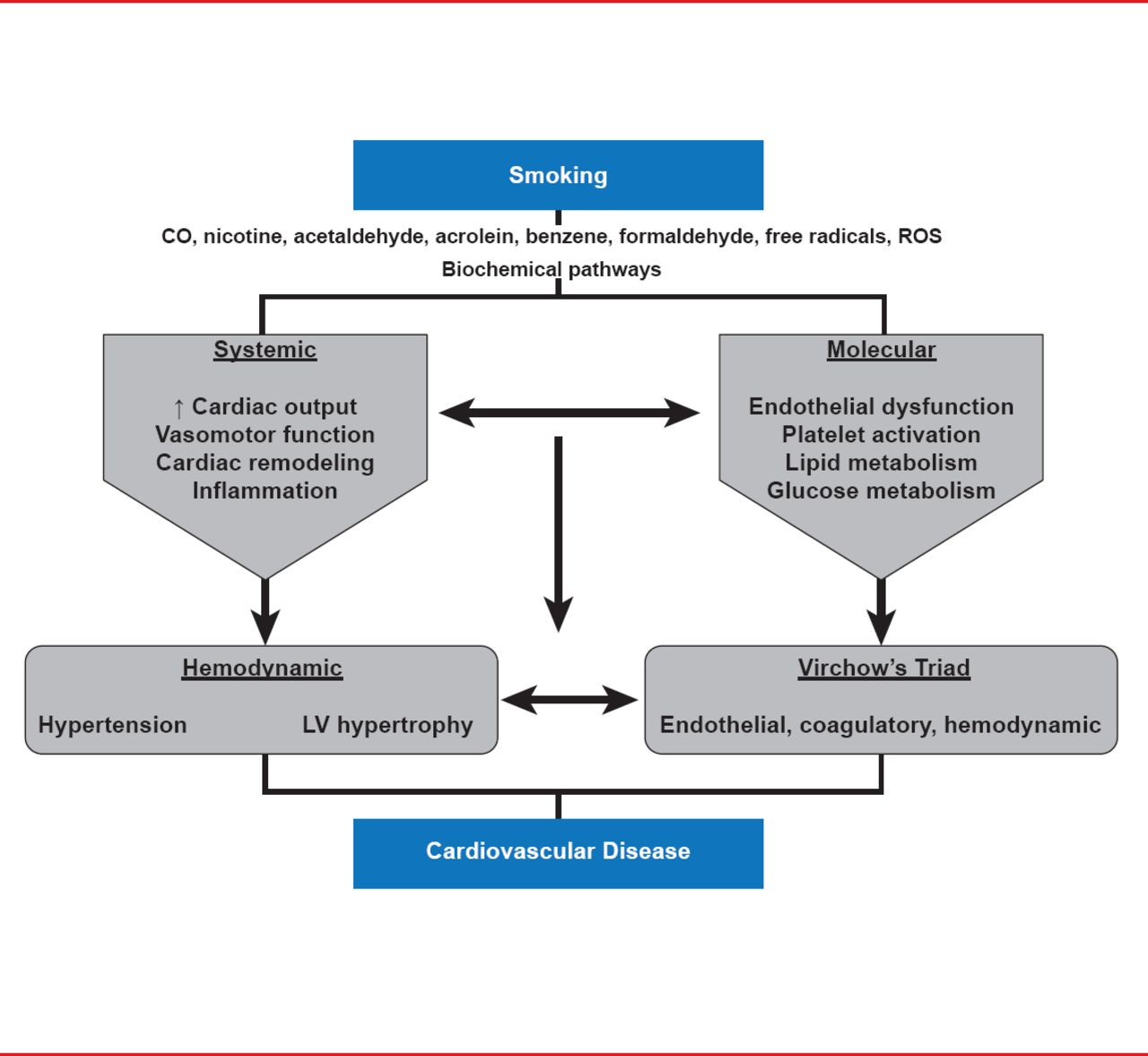
Pathways Linking Tobacco and CVD
CO=carbon monoxide; CVD=cardiovascular disease; LV=left ventricular; ROS=reactive oxygen species.
Reproduced from Kitami M and Ali MK. Tobacco, Metabolic and Inflammatory Pathways, and CVD Risk. Global Heart 2012;2(7):121–128. With permission from Elsevier.
IMPACT OF SECONDHAND SMOKE
Secondhand smoke causes ∼603,000 premature deaths annually, and 87% of secondhand smoking-related deaths are from ischemic heart disease [Oberg M et al. Lancet 2011]. A comprehensive literature review concluded that the CV effects of secondhand smoke are substantial and rapid, and that the effects of even brief exposure (minutes to hours) are often nearly as large (averaging 80% to 90%) as those of chronic active smoking [Barnoya J, Glantz SA. Circulation 2005]. Furthermore, they showed that long-term exposure to secondhand smoke at work or home is associated with a 30% increased risk for coronary heart disease (CHD) in adult nonsmokers.
SMOKING CESSATION AS A TREATMENT OF CVD
Smoking cessation is a powerful treatment for established CVD, reducing the risk of CV-related death by 36% and the risk of future cardiac event rates by 50%. These effects are comparable to the 15% to 35% reductions in CV-related death achieved with many widely used pharmacologic therapies (aspirin, β-blockers, ACE inhibitors, statins). Prof. Saade noted that tobacco cessation is one of the most important preventative measures available and that and no other preventive activity produces such significant results from such a small investment in time. The number needed to treat to prevent CV events or death is shown in Table 1.
Treating Tobacco Is Effective and Efficient for Reducing Cardiovascular Events and Death
Tobacco treatment is also cost-effective, with cessation counseling and medications costing $2587 per life-year saved [Cromwell J et al. Health Care Financ Rev 1997].
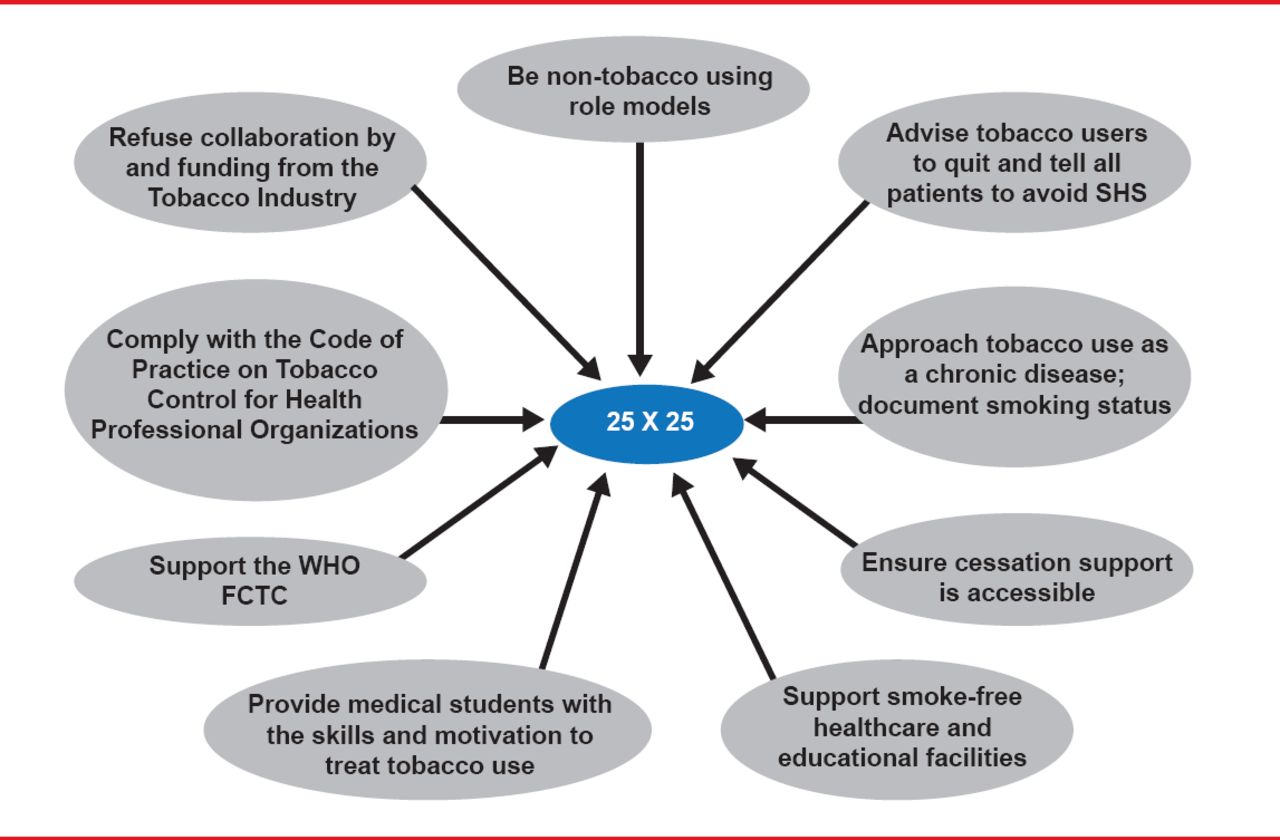
Prof. Saade noted that the cardiology team has a professional obligation to address tobacco use and exposure, and it is an essential component of CVD treatment for all patients. Cardiologists have an important role to play, as outlined in Figure 2, in achieving the “25 by 25” CVD goals established by the World Heart Federation.

Role of the Cardiologist to Achieve “25 by 25” CVD Goals
FCTC=Framework Convention on Tobacco Controls; SHS=secondhand smoke; WHO=World Healh Organization.
Reproduced with permission from GA Saade, MD.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.