

Summary
Carbohydrate counting has become the gold standard for adjusting prandial insulin dose despite limited evidence to recommend it over other dietary interventions for improving glycemic control in type 1 diabetes. This article discusses pooled data from six randomized controlled trials conducted over a 10-year period showing that carbohydrate counting had no significant effect on glycemic control.
- Diabetes & Endocrinology Clinical Trials
- Diabetes Mellitus Hyperglycemia/Hypoglycemia
- Diabetes & Endocrinology Clinical Trials
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
- Hyperglycemia/Hypoglycemia
Kirstine Bell, APD, CDE, University of Sydney, Sydney, Australia, presented pooled data from six randomized controlled trials conducted over a 10-year period showing that carbohydrate counting had no significant effect on glycemic control.
Carbohydrate counting has become the gold standard for adjusting prandial insulin dose despite limited evidence to recommend it over other dietary interventions for improving glycemic control in type 1 diabetes (T1D). Most international guidelines have based their recommendations on narrative reviews and the results of the few available studies; however, carbohydrate counting does not take into account differing effects of carbohydrates on blood glucose levels and the many different factors associated with stimulation of insulin secretion.
The objective of this meta-analysis was to assess the efficacy of carbohydrate counting on glycemic control in adults and children with T1D. Six studies that assessed the management of T1D with and without carbohydrate counting were included [DAFNE Study Group. BMJ 2002; Gilbertson HR et al. Diabetes Care 2001; Kalergis M et al. Diabetes Obes Metab 2000; Laurenzi A et al. Diabetes Care 2011; Scavone G et al. Diabet Med 2010; Trento M et al. J Endocrinol Invest 2011]. The control groups received usual care, general nutrition advice, or low glycemic index dietary advice. All studies were of at least 3 months' duration; patients (503 adults; 104 children aged 8 to 13 years) could be on flexible or fixed insulin therapy.
The primary outcome was improvement in glycated hemogloblin (HbA1C). Secondary measures included the number and severity of hypoglycemic episodes, fasting plasma glucose, insulin dose required to maintain glycemic control, body weight, and quality of life.
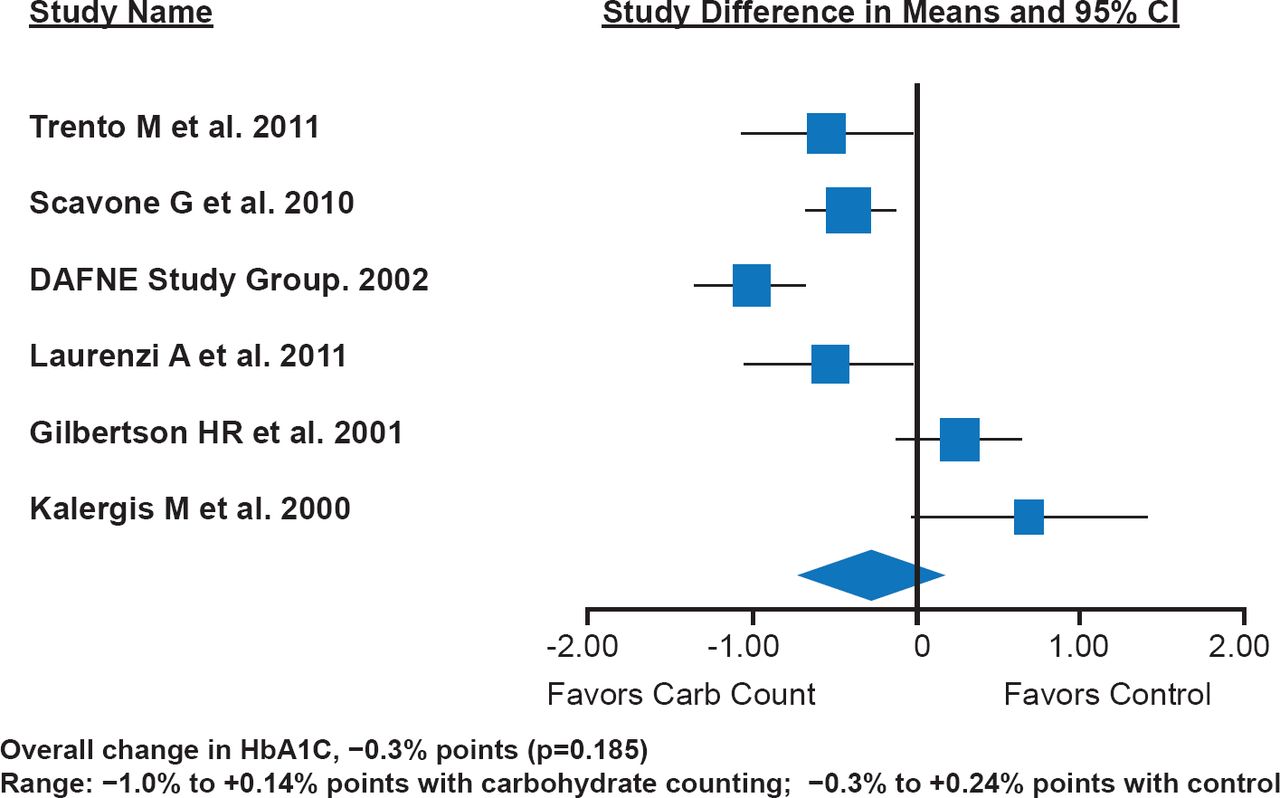
There was no significant improvement in HbA1C in patients who practiced carbohydrate counting compared with those who did not (Figure 1). The overall change in HbA1C was −0.3% points (p=0.185). Four studies favored carbohydrate counting (range, −1.0% to +0.14%); two favored the control (range, −0.3% to +0.24%).

Carbohydrate Counting Does Not Significantly Improve HbA1C
Reproduced with permission from K Bell, APD, CDE.
Due to the low number of studies and inconsistencies in reporting metrics, the results for the secondary outcomes are weak. However, there were trends for reduced risk of hypoglycemia, improved quality of life, and no changes in insulin dose, weight, or fasting plasma glucose level. The literature shows a wide variation in carbohydrate counting ability with greater accuracy and precision associated with lower HbA1C levels. However, skill and compliance were not measured in these studies.
As this analysis shows, carbohydrate counting may not result in optimal blood glucose control and clinicians need to realize some patients may fail with this approach. Many people with T1D have difficulty managing postprandial blood glucose levels despite their best efforts. In addition, carbohydrate counting has been linked to unhealthy food beliefs, fats and protein intake that exceed nutritional recommendations, and increased reliance on packaged foods. Clinicians need to emphasize healthy eating with insulin matched to food choices rather than choosing foods to limit insulin or making dosing easier. Additional research is needed to support the use of carbohydrate counting in clinical practice, particularly in children and adolescents. Recent studies examining the effect of protein and fat on insulin requirements show promising results and could provide an alternative method for determining prandial insulin dose.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.