

Summary
Although physicians have long subscribed to the fear that using intensive methods to lower the blood pressure of patients who had suffered acute intracerebral hemorrhage would result in increased risk of death or neurological deterioration, the technique is safe and effective, and should become the standard of care, according to results of the Second Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial [INTERACT2; NCT00716079; Anderson CS et al. N Engl J Med 2013].
- Cardiology Clinical Trials
- Ischemia
- Hypertensive Disease
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Ischemia
- Hypertensive Disease
Although physicians have long subscribed to the fear that using intensive methods to lower the blood pressure (BP) of patients who had suffered acute intracerebral hemorrhage (ICH) would result in increased risk of death or neurological deterioration, the technique is safe and effective, and should become the standard of care, according to results of the Second Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial [INTERACT2; NCT00716079; Anderson CS et al. N Engl J Med 2013].
While there was no reduction in deaths among acute ICH patients treated with an intensive BP-lowering strategy, functional outcomes and health-related quality of life (QoL) were better in these patients, according to John Chalmers, MD, PhD, Georgia Institute for Global Health, University of Sydney, Sydney, Australia, who presented the results of INTERACT2.
In the study, researchers examined the question of whether patients with acute ICH treated with the goal of reducing the BP to <140 mm Hg within an hour (early intensive group) or those treated with the goal of reducing BP to the current guideline-recommended goal of <180 mm Hg (standard group) would have improved survival free of major disability.
The study was performed across 144 hospitals in 21 countries. Patients (n=2839) with acute spontaneous ICH and systolic BP of 150 to 220 mm Hg were randomized within 6 hours of ICH to the early intensive (n=1403) or standard group (n=1436) and managed in-hospital for 7 days. The locally available intravenous BP-lowering agent used was based on the physician's choice.
Baseline characteristics of the two groups were similar and ∼68% of patients in each group were from China. The patient population had a mean age of 64 years, a mean BP of 179/101 mm Hg, and a median ICH volume of 11 mL.
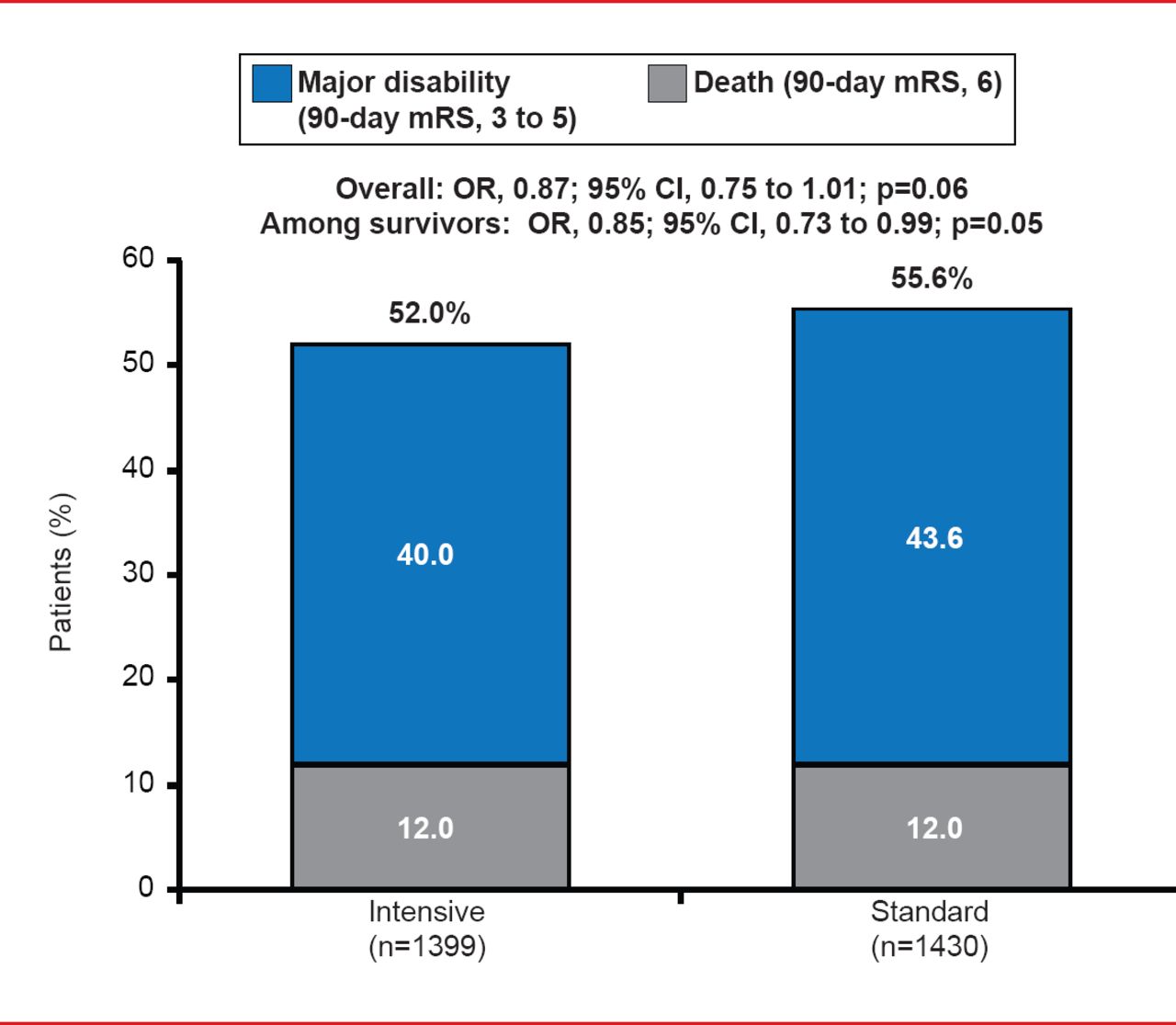
The occurrence of the primary composite outcome of death or major disability, defined as a 90-day modified Rankin Scale (mRS) score of 3 to 6, was nonsignificantly lower in the intensive group (52%) compared with the standard group (55.6%; OR, 0.87; 95% CI, 0.75 to 1.01; p=0.06; Figure 1). While the rate of death was similar in the two groups (∼12%), significantly fewer survivors in the early intensive group (40%) experienced major disability compared with the standard group (43.6%; p=0.05).

Death or Major Disability (90-day mRS Score, 3 to 6)
A prespecified subgroup analysis showed that the primary outcome findings did not significantly differ by region (ie, China vs other regions; p=0.97). Ordinal analysis of mRS score distribution showed that mRS scores were significantly lower in the intensive group versus the standard group (pooled OR for shift to higher mRS score, 0.87; 95% CI, 0.77 to 1.00; p=0.04).
Health-related QoL, measured using the European QoL-5 Dimensions (EQ-5D) questionnaire, was significantly better in the intensive group versus the standard group (overall health utility score, 0.60 vs 0.55; p=0.002; Figure 2). In particular, the intensive group had significantly fewer problems in the dimensions of self-care, usual activities, pain or discomfort, and anxiety or depression.

Health-Related Quality of Life
There were no significant differences between the groups in the secondary endpoints of median length of hospital stay (20 vs 19 days; p=0.43), 90-day institutional care (9% for both), 24-hour neurological deterioration (66% vs 68%, p=0.22), severe hypotension (0.5% vs 0.6%, p=0.83), nonfatal serious adverse events (23.3% vs 23.6%; p=0.92), and cause-specific mortality.
INTERACT2 findings show that early aggressive BP lowering in acute ICH patients is generally safe and effective compared with standard therapy, and may yield better functional outcomes.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.