

Summary
Nocturnal noninvasive ventilation (nNIV) is used for treatment of multiple pathologies such as neuromuscular disorders, sleep apneas, restrictive thoracic disorders, chronic obstructive pulmonary disease, and obesity-hypoventilation syndrome with the goals of increasing gas exchange, decreasing respiratory muscle fatigue, decreasing stress, and increasing comfort and sleep. This article discusses the basics of nNIV and highlighted areas of emerging research and new challenges in the field, the use of nNIV in patients with heart failure that have sleep-disordered breathing, the efficacy of different modes of bilevel nNIV in patients with obesity hypoventilation syndrome, and the use of nNIV in patients with neuromuscular disorders.
- Lower Respiratory Infections
- Heart Failure
- Obesity
- Sleep Disorders
- Chronic Obstructive Pulmonary Disease
- Lower Respiratory Infections
- Heart Failure
- Obesity
- Sleep Disorders
- Chronic Obstructive Pulmonary Disease
- Pulmonary & Critical Care
Nocturnal noninvasive ventilation (nNIV) is used for treatment of multiple pathologies such as neuromuscular disorders, sleep apneas, restrictive thoracic disorders, chronic obstructive pulmonary disease (COPD), and obesity-hypoventilation syndrome with the goals of increasing gas exchange, decreasing respiratory muscle fatigue, decreasing stress, and increasing comfort and sleep. Sairam Parthasarthy, MD, University of Arizona, Tucson, Arizona, USA, presented on the basics of nNIV and highlighted areas of emerging research and new challenges in the field.
Positive airway pressure (PAP) results in greater thoracic and lung volume, which leads to increased cardiac output, reduced venous return, and reducing afterload [Antonescu-Turcu A, Parthasarthy S. Respir Care 2010]. Despite such favorable physiological effects, continuous PAP (CPAP) therapy resulted in a similar rate of transplantation-free survival, as compared with a control group [Bradley TD et al. N Engl J Med 2005]. Dr. Parthasarthy said that such a finding may be due to residual central sleep apnea despite CPAP therapy and that a different method of respiratory support, called adaptive servo-ventilation (ASV) can significantly reduce central sleep apnea when compared with control populations in patients with heart failure [Teschler H et al. Am J Resp Crit Care Med 2001; Morgenthaler TI et al. Sleep 2007; Arzt M et al. Chest 2008; Javaheri S et al. Sleep 2011]. Such amelioration of central sleep apnea was observed across various manufacturers of these devices and across a variety settings.
Dr. Parthasarthy also addressed the question of how to determine the target tidal volume in patients with nocturnal hypoventilation and challenges that may prevent achieving the target. For example, an air leak tracing during polysomnography can indicate the degree of air-leak present during NIV titration, and that such an air-leak can reduce patient adherence due to diminished performance of the system [Valentin A et al. Sleep 2011].
Stefano Nava, MD, Bologna University Hospital Authority St. Orsola-Malpighi Polyclinic, Bologna, Italy, discussed the controversial issue of nNIV use in patients with COPD and overlap syndrome (COPD and sleep apnea). Prof. Nava pointed out that, at the present time, the long-term use of nNIV is not recommended in COPD patients for the treatment of chronic respiratory failure due to several evidence-based factors. A recent study demonstrated that chronic nNIV did not improve mortality in patients with COPD [Shi JX et al. Chin Med J (Engl) 2013] and another study demonstrated a significant trend in decreased mortality with nNIV treatment [McEvoy RD et al. Thorax 2009]. In addition, Prof. Nava highlighted a meta-analysis that analyzed other parameters such as sleep efficiency, CO2 partial pressure, forced expiratory volume and forced vital capacity (FVC) reported no significant difference in mortality with nNIV treatment, as compared with long-term oxygen therapy [Wijkstra PJ et al. Chest 2003].
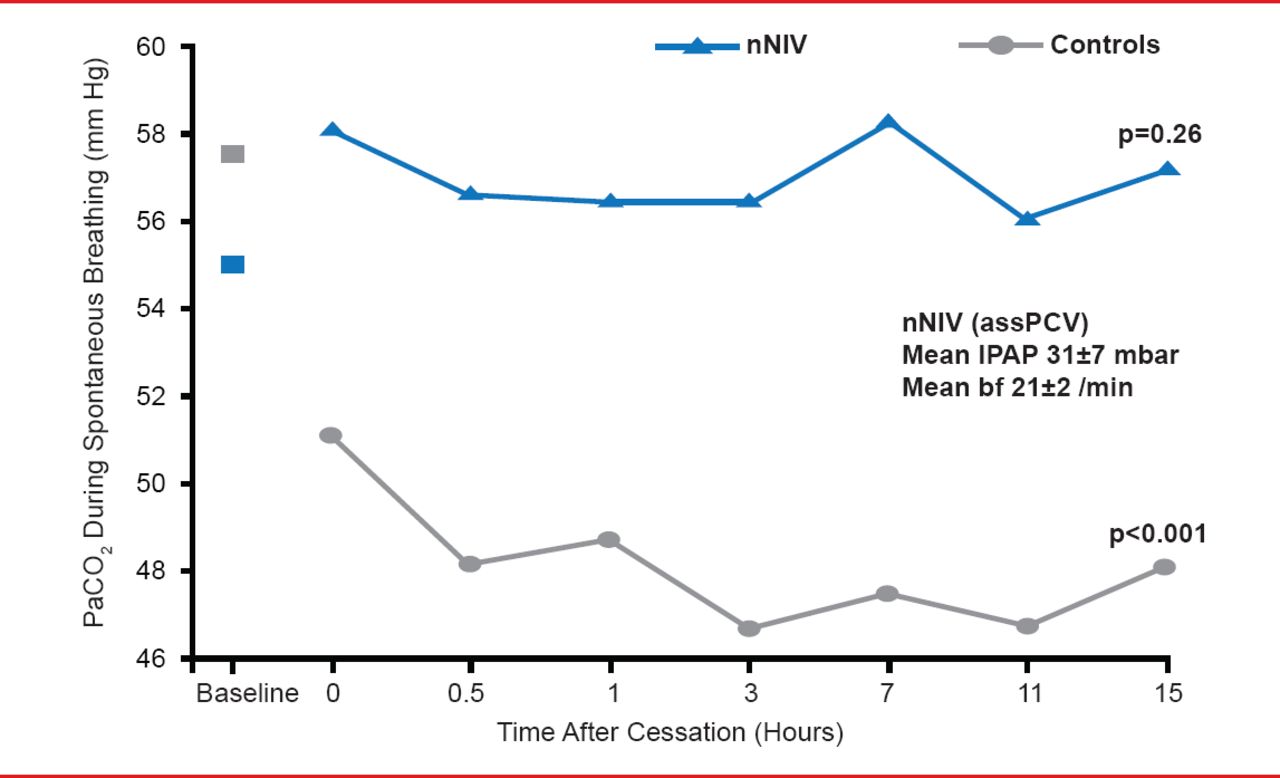
Prof. Nava suggested that one reason that few COPD patients respond to nNIV may be setting related. The three largest trials reported in the literature that demonstrated no benefit with nNIV treatment used an inspiratory PAP (IPAP) and expiratory PAP (EPAP) of 12 cm H2O and 4 cm H2O [Casanova C et al. Chest 2000], and 14 cm H2O and 2 cm H2O [Clini E et al. Eur Respir J 2002]; whereas a study that demonstrated nNIV benefit used an IPAP and EPAP of 13 cm H2O and 5 cm H2O [Mc Evoy RD et al. Thorax 2009]. Prof. Nava highlighted a study that used more aggressive pressures with an IPAP of 31 mm Hg that resulted in a significantly lower partial pressure of CO2 during spontaneous breathing after the discontinuation of nNIV (Figure 1) [Windisch W et al. Respir Physiol Neurobiol 2006]. This approach however may harm the cardiovascular system, since when compared with lower levels of IPAP, the “German approach” resulted in a significant reduction in cardiac output [Lukácsovits J et al. Eur Respir J 2012].

Aggressive IPAP in nNIV Decreases CO2 Partial Pressure in Patients With COPD
nNIV=nocturnal noninvasive ventilation; IPAP=inspiratory positive airway pressure.
Reproduced from Windisch W et al. Nocturnal non-invasive positive pressure ventilation: Physiological effects on spontaneous breathing. Respir Physiol Neurobiol 2006;150(2–3):251–260. With permission from Elsevier.
Finally, Prof. Nava pointed out that patients with overlap syndrome appear to respond well to nNIV. Several studies demonstrated a significant increase in survival rates in patients with overlap syndrome that were treated with CPAP, as compared with overlap syndrome patients not treated with CPAP and COPD patients [Kouns A, Philips B. Curr Treat Options Neurol 2011].
S. Javaheri, MD, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA, discussed the use of nNIV in patients with heart failure that have sleep-disordered breathing. The benefits of ASV devices include their ability to automatically vary the inspiratory support, automatic CPAP to prevent obstructive events from occurring, and automatic back-up rate to prevent apnea.
ASV devices can automatically increase inspiratory support during hypopneas and decrease support during hyperpnea. Dr. Javaheri pointed out that this feature is important in patients with heart failure as the mechanisms that underlie periodic breathing and central sleep apnea in these patients is oscillations in ventilatory drive. ASV devices decrease these oscillations. In addition, ASV devices also initiate a mandatory breath on a timed basis, aborting the course of an impending apnea. Finally, the expiratory pressure prevents upper airway closure and eliminates obstructive events. In the new generation of auto ASV devices, the expiratory pressure varies automatically in a similar fashion to auto CPAP devices. These three features of ASV devices, autoinspiratory pressure support, auto CPAP and auto back-up rate make ASV devices most appropriate for mixed/hybrid sleep-disordered breathing consisting both of central sleep apnea, obstructive sleep apnea and hypopneas, provided that these events were not all eliminated by the use of CPAP.
In a study of patients with complex sleep apnea and some with Hunter-Cheyne-Stokes breathing with central sleep apnea, Dr. Javaheri pointed out that patients experienced the greatest benefit with auto ASV and auto ASV advanced, as compared with CPAP [Javaheri S et al. Sleep 2011].
Meanwhile multiple studies have been performed in patients with heart failure with various ASV devices. In their meta-analysis, Sharma and associates [Chest 2012] included studies of ≥1 week duration comparing ASV to a control condition (which was subtherapeutic ASV, CPAP, bilevel positive airway pressure, oxygen therapy, or no treatment) in adult heart failure patients with sleep apnea. Comparing ASV to control conditions, the weighted mean difference in apnea hyponea index (AHI; −15 events/hour; 95% CI, −21.03 to −8.25) significantly favored ASV. Importantly, when the crossover studies were compared, AHI decreased from baseline of about 50 events per hour to 6 per hour with ASV compared with 21 per hour in control conditions.
These data provide a compelling rationale for large-scale randomized controlled trials to assess the clinical impact of ASV on mortality in heart failure patients. Currently two trials are ongoing.
Amanda Piper, PhD, Royal Prince Alfred Hospital, Camperdown, Australia, discussed the efficacy of different modes of bilevel nNIV in patients with obesity hypoventilation syndrome (OHS). In a study of 36 OHS patients with moderate to severe upper airway obstruction randomized to CPAP or bilevel support in spontaneous mode for 3 months, similar clinical outcomes were achieved delete period [Piper AJ et al. Thorax 2008].
A more recent study compared bilevel support in spontaneous versus spontaneous timed (S/T) mode [Contal O et al. Chest 2013]. In this study, 10 patients with OHS were randomized to spontaneous mode, S/T mode with a low back-up respiratory rate (BURR), or S/T mode with a high BURR over 3 nights. A greater number of respiratory events occurred in patients treated with spontaneous mode, compared with either of the S/T mode, raising the issue of whether the spontaneous mode should be used in this population. However, Prof. Piper pointed out that the study included only a small number of patients naïve to nNIV therapy with settings not titrated to the mode used. Nevertheless, data from other studies suggests more passive ventilation in this population may yield greater clinical benefits. Prof. Piper also discussed the use of volume targeted pressure support in OHS, with a recent large study finding no additional clinical benefit of this mode over standard bilevel therapy in routine practice [Murphy PB et al. Thorax 2012].
Prof. Piper also highlighted the importance of titrating inspiratory support to achieve an adequate tidal volume. For patients with OHS, 8 to 10 mL/kg of ideal body weight appears to be a good nocturnal tidal volume target [Murphy PB et al. Thorax 2012; Budwesier S et al. J Intern Med 2007].
Amy Atkeson, MD, Columbia University College of Physicians & Surgeons, New York, New York, USA, discussed the use of nNIV in patients with neuromuscular disorders. The rationale for treating patients with neuromuscular disorders with nNIV is that it may help rest overtaxed respiratory muscles, improvement of muscle strength and contractility, improvement in respiratory mechanics, and recruitment of atelectatic and partially atelectatic alveoli.
Early initiation of nNIV therapy in patients with neuromuscular disorders, such as ALS, may confer a survival advantage. Dr. Atkeson highlighted several studies that demonstrated a reduced decline in FVC [Kleopa KA et al. J Neurol Sci 1999] and cost-effectiveness [Gruis KL et al. Health Serv Res 2005]. However, Dr. Atkeson pointed out that although the evidence is generally positive, it is weak and more research is required to determine the optimal use of nNIV in patients with neuromuscular disorders.
Although additional research is required in many cases to determine the benefit and/or optimal use of nNIV in conditions that cause sleep disorder, nNIV appears to offer the promise of improved outcomes in patients with sleep disorders.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.