

Summary
The impact of obesity on many chronic diseases is well known, but the effect of obesity on clinical outcomes for people with chronic obstructive pulmonary disease (COPD) is less clear. The number of people with COPD who are obese is expected to increase in line with the obesity pandemic, making it essential to gain a better understanding of the effects of obesity on COPD. Although classically considered a wasting disease, a link between COPD and obesity is becoming increasingly recognized, and it may influence clinical diversity in COPD.
- Pulmonary Clinical Trials
- Chronic Obstructive Pulmonary Disease
- Obesity
- Pulmonary & Critical Care
- Pulmonary Clinical Trials
- Chronic Obstructive Pulmonary Disease
- Obesity
- Featured Meeting - Specialty page
The impact of obesity on many chronic diseases is well known, but the effect of obesity on clinical outcomes for people with chronic obstructive pulmonary disease (COPD) is less clear. The number of people with COPD who are obese is expected to increase in line with the obesity pandemic, making it essential to gain a better understanding of the effects of obesity on COPD.
Although classically considered a wasting disease, a link between COPD and obesity is becoming increasingly recognized, and it may influence clinical diversity in COPD, said Frits M. E. Franssen, MD, PhD, CIRO+, Center of Expertise for Chronic Organ Failure, Horn, The Netherlands. Data on the prevalence of obesity in COPD have conflicted, with some studies showing a higher prevalence among patients with COPD and others showing a lower prevalence [Vozoris NT, O'Donnell DE. Can Respir J 2012; Montes de Oca M et al. Respir Med 2008; Steuten LM et al. Prim Care Respir J 2006; Eisner MD et al. Respir Res 2007]. Low levels of physical activity have been consistently reported for patients with COPD, and this may contribute to weight gain.
Contrary to expectations, obesity is not necessarily associated with worse patient-related outcomes in COPD, said Prof. Franssen. He pointed to an early study in which the risk of mortality was evaluated in obese and normal-weight patients with COPD [Landbo C et al. Am J Respir Crit Care Med 1999]. The relative risk of all-cause mortality was increased for obese patients with mild or moderate COPD compared with normal-weight patients. However, in contrast to patients with mild and moderate COPD, among patients with severe disease, the risks of all-cause and COPD-related mortality were lowest for obese patients. These findings are referred to as the obesity paradox.
Studies have also found different effects of obesity on dyspnea. In one study, obese patients with COPD reported increased dyspnea and poorer health-related quality of life than normal-weight patients, even though lung function was better for obese and overweight patients [Cecere LM et al. COPD 2011]. In another study, researchers found that absolute peak workload increased in obese patients during cycling (compared with normal-weight patients matched for age and degree of airway obstruction), but these patients reported less dyspnea during all levels of ventilation during cycling [Ora J et al. Am J Respir Crit Care Med 2009].
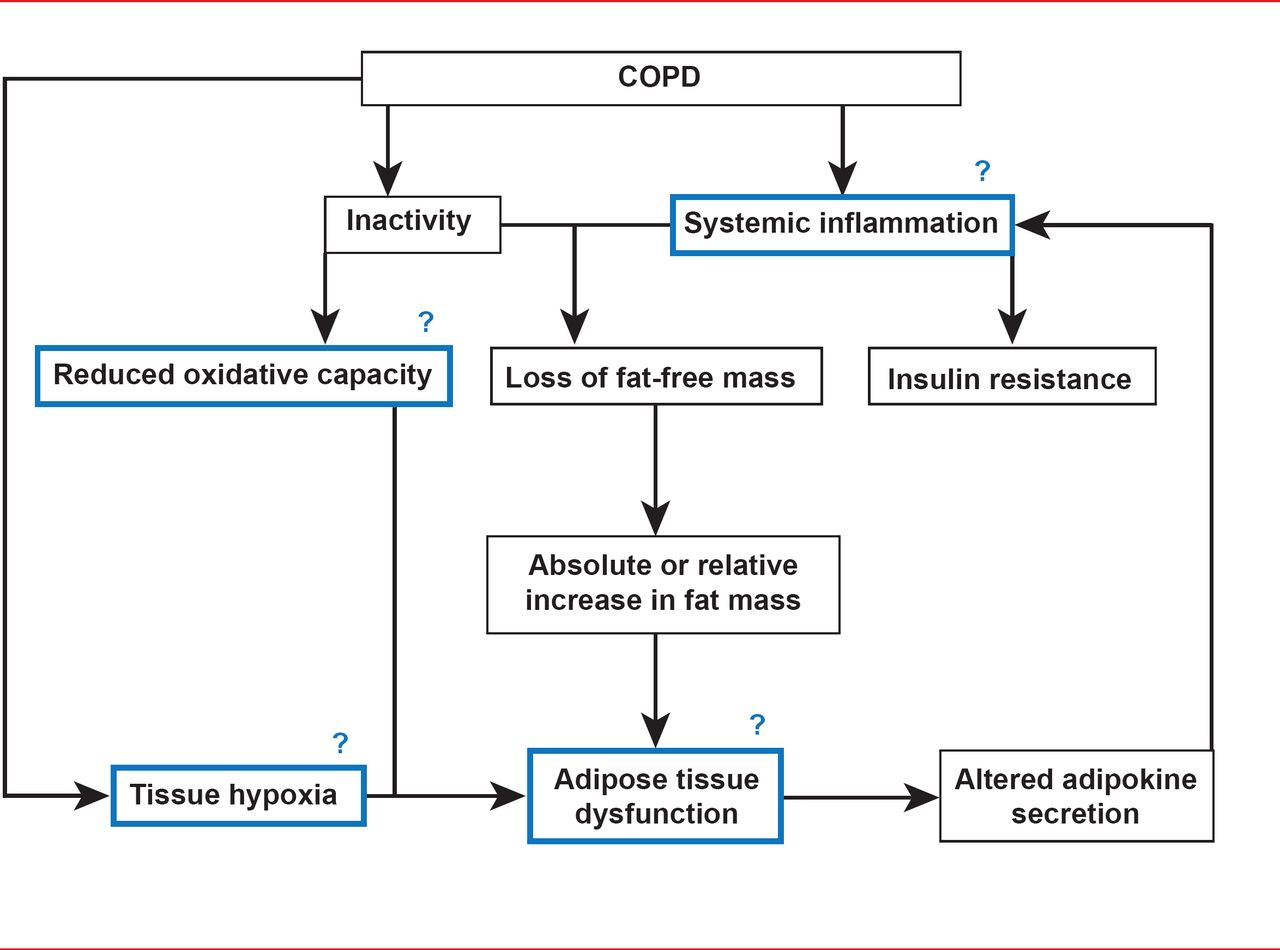
Obesity appears to be a substantial contributor to systemic inflammation in COPD. Adipose tissue is a source of inflammation in obesity, and obesity (high body mass index [BMI]) has been associated with highly elevated levels of C-reactive protein in patients with COPD; the highest levels have been found in patients with abdominal obesity [Breyer MK et al. Clin Nutr 2009]. In addition, persistent inflammation in COPD has been associated with a high BMI but not with the fat-free mass index, which suggests a role for adipose tissue in the inflammatory process [Agusti A et al. PloS One 2012; van den Borst B et al. Am J Respir Crit Care Med 2013]. Prof. Franssen said that increasing evidence suggests a relationship between visceral adipose tissue dysfunction and the pathophysiology of COPD, and he proposed several links between COPD, adipose tissue dysfunction, and systemic inflammation, noting that several questions remain unanswered (Figure 1) [Franssen FME et al. Thorax 2008].

Obesity and Chronic Obstructive Pulmonary Disease: Unanswered Questions
Reproduced from Franssen FME et al.
Obesity and the Lung: 5 • Obesity and COPD. Thorax 2008;23(12):1110–1117. With permission from The BMJ Publishing Group.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.