

Summary
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a safe, accurate, and minimally invasive test for sarcoidosis. This article reviews the role of bronchoscopy, and in particular of EBUS-TBNA, for diagnosis of sarcoidosis.
- Lower Respiratory Infections
- Lymphatic Diseases
- Pulmonary & Critical Care
- Lower Respiratory Infections
- Lymphatic Diseases
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a safe, accurate, and minimally invasive test for sarcoidosis. Rocco Trisolini, MD, Maggiore Hospital, Bologna, Italy, reviewed the role of bronchoscopy, and in particular of EBUS-TBNA, for diagnosis of sarcoidosis.
The first aspect Prof. Trisolini pointed out is that bronchoscopy with its sampling procedures, including EBUS-TBNA, cannot diagnose sarcoidosis. Sarcoidosis has the highest probability of being diagnosed correctly if the clinical and radiological data are supported by the pathological evidence of noncaseating granulomatous inflammation, and alternative causes of granulomatous inflammation are ruled out. Bronchoscopy can only provide the pathologic evidence of granulomatous inflammation, which is nonspecific to sarcoidosis both in the lung and in the mediastinum. Studies have demonstrated that non-necrotizing granulomas indistinguishable from those seen in sarcoidosis can be retrieved with EBUS-TBNA or endoscopic US-NA in 34% to 37% of patients with tuberculosis lymphadenitis [Puri R et al. Endoscopy 2010; Navani N et al. Thorax 2011]. As a consequence, bronchoscopy (and EBUS-TBNA) can only provide a piece of evidence in the clinical process that ultimately leads to the diagnosis of sarcoidosis or rules it out.
This said, if the clinical and radiological data are not strong enough to confirm a diagnosis of sarcoidosis on clinical grounds, Prof. Trisolini maintains that the bronchoscopy procedures aimed at sampling the mediastinum (conventional [c-TBNA] and especially EBUS-TBNA) are associated with the best performance characteristics. The intrathoracic lymph node involvement in sarcoidosis is more common than lung involvement in imaging studies [Baughman RP. Am J Resp Crit Care Med 2011], and the success rate of transbronchial lung biopsy is very low in the absence of lung involvement. The pattern of lymphadenopathy is also very favorable to a bronchoscopy diagnosis as the lymph node stations preferred for EBUS-TBNA and c-TBNA are also those which are more frequently involved in sarcoidosis and which harbor the largest lymph nodes (4R, 7, and 11) [Trisolini R et al. Respir Med 2013].
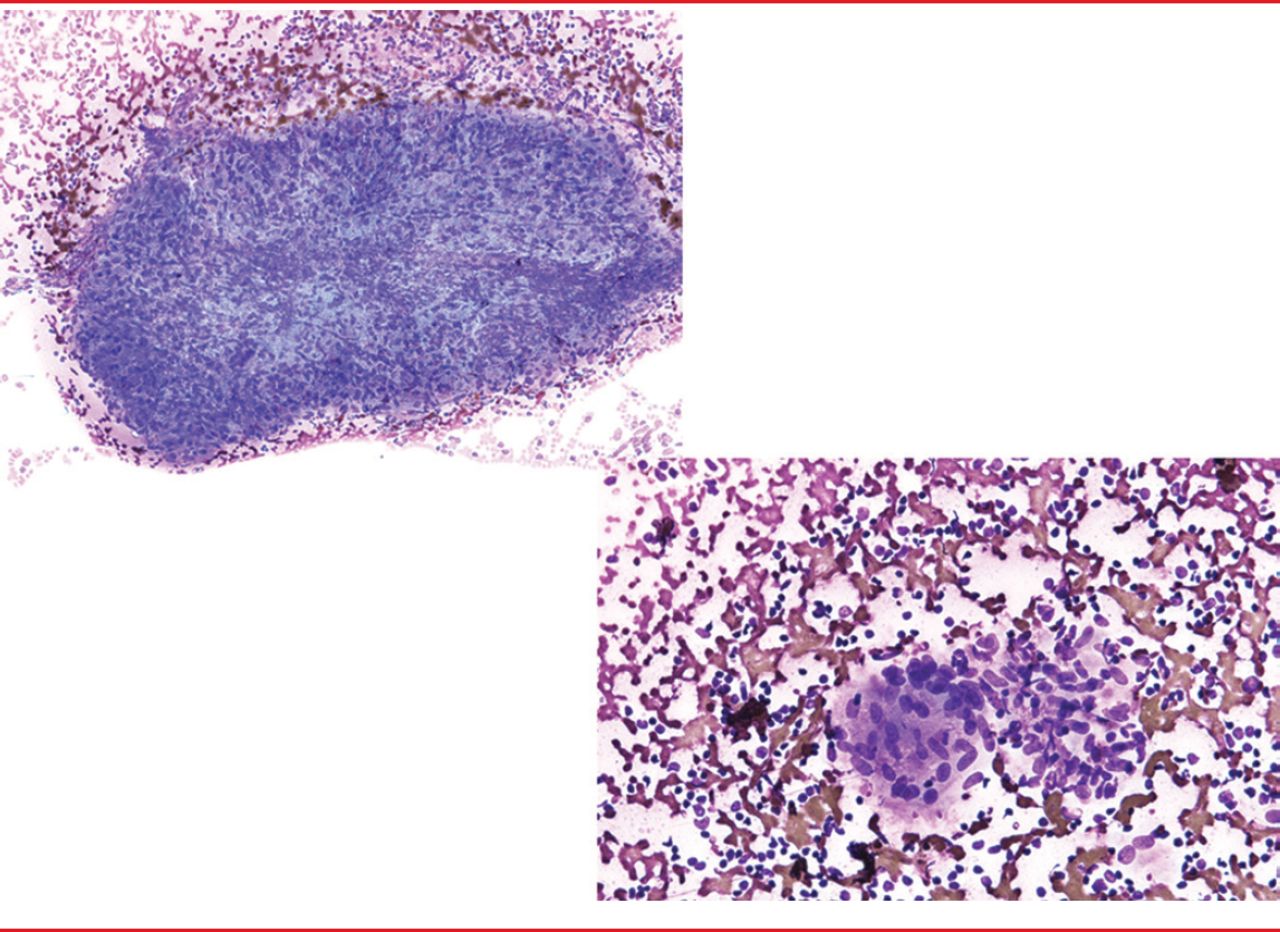
Once the decision to perform EBUS-TBNA or c-TBNA to sample the mediastinum of a patient with suspected sarcoidosis has been made, some factors which can predict the yield of such sampling procedures should be considered. The first factor is the so called “pathologist factor”. Tremblay A et al. [Chest 2009] demonstrated, the superiority of EBUS-TBNA versus c-TBNA in sarcoidosis, and that when the same slides from the same patients are independently interpreted the yield granulomas can be quite different. The preparation method (smears, cell-blocks, Thin-Prep, cytospins) of the cytologic material retrieved with EBUS-TBNA or c-TBNA can also play a role. Cancellieri A et al. [Respiration 2013] described the cytomorphology of granulomas on smears prepared from material retrieved with TBNA and suggested that the diagnosis of granulomas on smears is easy and reliable (Figure 1). The second with influence over the yield of EBUS-TBNA and c-TBNA in sarcoidosis is the number of lymph node stations that are sampled (the more the better). The importance of this factor was demonstrated in the studies by Trisolini R et al. where a positive diagnosis was made in 92.5% of patients with two nodes sampled versus 65% in patients with only one node sampled (p=0.01) [J Thorac Cardiovasc Surg 2008]. An alternative to sampling multiple nodes to optimize the yield of EBUS-TBNA is the use of rapid on-site evaluation. The evidence of non-necrotizing granulomas at on-site assessment might obviate the need for further sampling in the appropriate clinical-radiological context.
EBUS-TBNA and c-TBNA in sarcoidosis have been studied primarily in populations with a high prevalence of the disease and, therefore, with high pre-test probability. It remains to be seen whether the performance characteristics of EBUS-TBNA would be similar in study populations with a low-prevalence of the disease.

Granulomas.
Reproduced from Trisolini R et al. Transbronchial needle aspiration in sarcoidosis: Yield and predictors of a positive aspirate. J Thorac Cardiovasc Surg 2008;135(4):837–842. With permission from Elsevier.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.