

Summary
In 2012, the American Heart Association (AHA), American College of Cardiology (ACC), and the Heart Rhythm Society (HRS) published updated clinical practice guidelines for the management of cardiac resynchronization therapy (CRT) [Tracy CM et al. Circulation 2012]. The new guideline proposes several changes in recommendations for CRT, compared with the 2008 guideline, and this article discusses the most significant changes.
- Arrhythmias
- Cardiology Guidelines
- Heart Failure
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Arrhythmias
- Cardiology Guidelines
- Heart Failure
- Interventional Techniques & Devices
- Exclusive Article - For home page
In 2012, the American Heart Association (AHA), American College of Cardiology (ACC), and the Heart Rhythm Society (HRS) published updated clinical practice guidelines for the management of cardiac resynchronization therapy (CRT) [Tracy CM et al. Circulation 2012].
The new guideline proposes several changes in recommendations for CRT, compared with the 2008 guideline. The most significant changes are
-
▪ Limitation of the Class I indication to patients with QRS duration ≥150 ms
-
▪ Limitation of the Class I indication to patients with left bundle branch block (LBBB)
-
▪ Expansion of Class I indication to NYHA Class II (and with LBBB with QRS duration ≥150 ms)
-
▪ Addition of a Class lib recommendation for patients who have left ventricular ejection fraction ≤30%, ischemic etiology of heart failure (HF), sinus rhythm, LBBB with a QRS duration ≥150 ms, and NYHA Class I symptoms.
The AHA/ACC/HRS guidelines recommend CRT over medical therapy for the treatment of HF patients based on evidence from multiple trials. Mark Link, MD, Tufts University School of Medicine, Boston, Massachusetts, USA, highlighted several trials that specifically analyzed results for patients with LBBB or non-LBBB. In the CARE-HF trial, 813 HF patients were randomized to receive CRT or medical therapy with a mean follow-up time of 29.4 months [Cleland JG et al. N Engl J Med 2005]. The primary endpoint of death or unplanned hospitalization in the cardiac synchronization arm was 39%, compared with 55% in the medical therapy arm (HR, 0.63; 95% CI, 0.51 to 0.77; p<0.001).
In the RAFT trial, 1798 patients were randomized to receive an implantable cardioverter-defibrillator (ICD) alone or an ICD in combination with CRT and followed for a mean of 40 months [Tang AS et al. N Engl J Med 2010]. The primary endpoint of death or hospitalization was reached by 33.2% of patients in the ICD plus CRT arm, as compared with 40.3% of patients in the ICD arm (HR, 0.075; 95% CI, 0.64 to 0.87; p<0.001) for the ICD plus CRT arm. In the MADIT-CRT trial, 1820 patients were randomized 3:2 to receive an ICD plus CRT or an ICD only and were followed for a mean of 2.4 years [Moss AJ et al. N Engl J Med 2009]. The primary endpoint of death or hospitalization was reached by 17.2% of patients in the ICD plus CRT arm, as compared with 25.3% in the ICD-only arm (HR, 0.66; 95% CI, 0.52 to 0.84; p=0.001). Dr. Link pointed out that in all of these trials, LBBB and/or the QRS duration of 150 ms or longer was extremely important in determining patient benefit of CRT treatment [Cleland JG et al. N Engl J Med 2005; Tang AS et al. N Engl J Med 2010; Moss AJ et al. N Engl J Med 2009].
Lynne Warner Stevenson, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed the importance of HF classification in regards to CRT. Dr. Stevenson pointed out that although CRT has been demonstrated to be beneficial for many patients, those patients with advanced Class IV HF do not appear to benefit from CRT, particularly if they have received inotropic therapy [Bhattacharya S et al. J Card Fail 2010]. However, she emphasized the strength of data that supports use of CRT to decrease disease progression in patient with Class II symptoms. As an HF clinician, she pointed out the difficulty of distinguishing between Class I and Class II symptoms, which may become less relevant as LBBB is increasingly appreciated as a cause, not just a result, of worsening heart failure.
Ibrahim Almasry, MD, Stony Brook Heart Rhythm Center, Stony Brook, New York, USA, discussed the importance of QRS duration in CRT therapy. Longer QRS duration and width of QRS are associated with poorer HF outcomes, including total mortality [Kashani A et al. J Am Coll Cardiol 2005; Bleeker GB et al. J Cardiovasc Electrophysiol 2004]. In the REVERSE trial, only patients with QRS duration of at least 152 ms experienced a benefit from CRT. Dr. Almasry noted that in the MADIT-CRT trial, patients with QRS duration of at least 150 ms experienced a benefit from CRT, whereas patients with QRS duration of <150 ms did not [Moss AJ et al. N Engl J Med 2009]. Similar findings were demonstrated in the RAFT trial; however, patients with a paced QRS duration of 200 ms or longer did not receive benefit from CRT [Tang AS et al. N Engl J Med 2010].
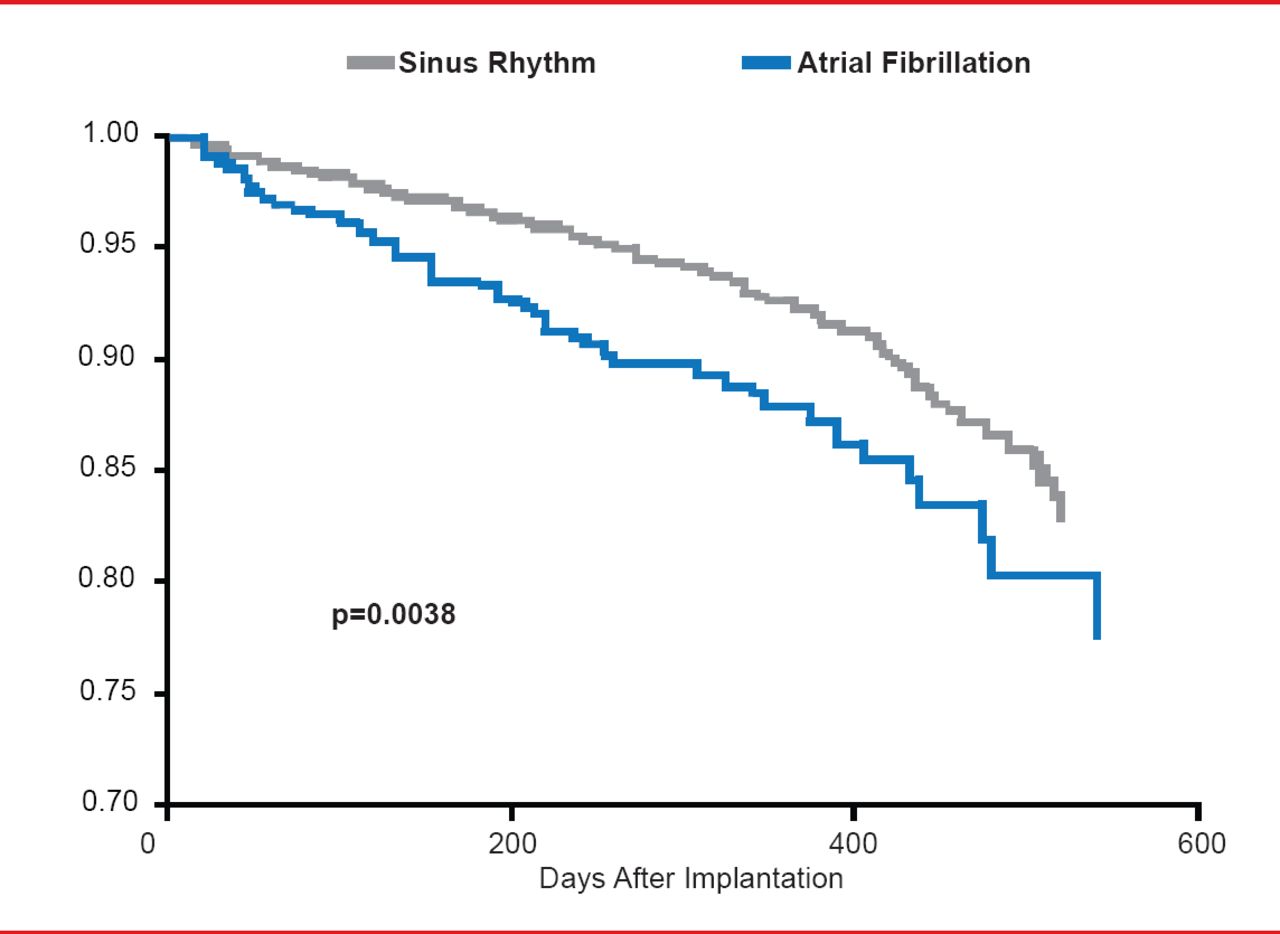
Derek Exner, MD, MPH, Libin Cardiovascular Institute of Alberta, Calgary, Alberta, Canada, discussed CRT in patients with atrial fibrillation (AF), which is common in patients with HF. Multiple trials have demonstrated that patients with AF tend to respond less to therapy and have a greater annual mortality rate, as compared with patients with sinus rhythm [Wilton SB et al. Heart Rhythm 2011]. In addition, patients with AF are more likely to experience mortality following CRT than patients without AF(p=0.0038; Figure 1) [Bogale N et al. Eur J Heart Fail 2012].

Patients With Atrial Fibrillation Experience Greater Risk of Death Following CRT
CRT=cardiac resynchronization therapy.
Reproduced from Bogale N et al. The European CRT Survey: 1 year (9–15 months) follow-up results. Eur J Heart Failure 2012;4(1):61–73. With permission from Oxford University Press.
Whether the benefits observed with CRT are similar in patients with versus without AF is unclear. A meta-analysis of 23 observational studies by Wilton et al. found that AF was associated with an increased risk of nonresponse to CRT (34.5% vs 26.7%; pooled relative risk [RR] 1.32; 95% CI, 1.12 to 1.55; p=0.001) and all-cause mortality (10.8% vs 7.1% per year; pooled RR 1.50; 95% CI, 1.08 to 2.09; p=0.015) [Wilton SB et al. Heart Rhythm 2011]. The percentage of biventricular pacing (BiV) that is required for optimal survival rates appears to be >98.47%, as reported by an observational study [Hayes DL et al. Heart Rhythm 2011]. In the AF subset in the RAFT trial, there was no significant difference in the primary endpoint between patients that received an ICD plus CRT or an ICD alone (HR, 0.96; 95% CI, 0.65 to 1.41;p=0.82) [Healey et al. Circ Heart Fail 2012]. However, Dr. Exner pointed out that the BiV in the RAFT trial was inadequate, as ∼47% of AF patients had a BiV of ∼90%. Dr. Exner concluded by stating that there is questionable benefit of CRT in patients with AF, although a higher BiV may improve outcomes, and additional randomized controlled trials are required.
Pamela Karasik, MD, Georgetown University, Washington, District of Columbia, USA, presented the updates to the AHA/ACC/HRS guidelines for CRT in HF patients who require pacing. Several studies, including the more recent MADIT-CRT and RAFT, have demonstrated that a greater frequency of pacing is associated with worsening HF and greater mortality [Sweeney MO et al. Circulation 2003; Steinberg JS et al. J Cardiovasc Electrophysiol 2005; Tang AS et al. N Engl J Med. 2010].
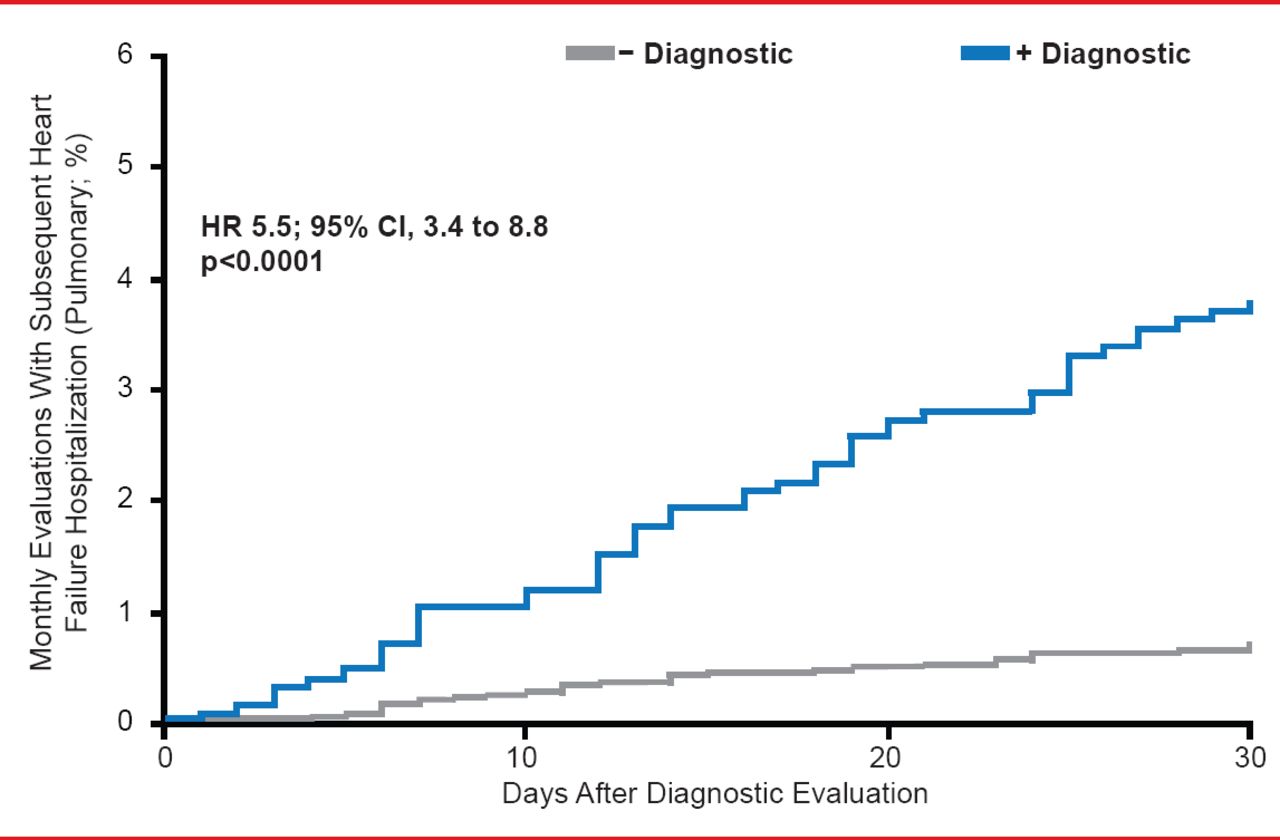
Amit Shanker, MD, Columbia University College of Physicians and Surgeons, New York, New York, USA, discussed the in-person and remote monitoring of patients with HF that have received CRT. The PARTNERS HF trial demonstrated that patients at risk of HF-associated hospitalization could be effectively identified by an integrated diagnostic algorithm (Figure 2) [Whellan DJ et al. J Am Coll Cardiol 2010]. Dr. Shanker highlighted that patients prefer remote monitoring over in-clinic follow-ups and there is an improvement in operational efficiency, which ultimately leads to lower costs.

Combined Device Diagnostics Can Accurately Predict Heart Failure Patients at Risk for Hospitalization
Reproduced from Whellan DJ et al. Combined Heart Failure Device Diagnostics Identify Patients at Higher Risk of Subsequent Heart Failure Hospitalizations. J Am Coll Cardiol 2010;55(17):1803. With Permission from Elsevier.
Bruce Wilkoff, MD, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, Ohio, USA, discussed the current gaps in evidence for CRT. Although there are areas where evidence is strong for the use of CRT, such as in patients with a QRS ≥150 ms and the presence of LBBB, there are other areas where evidence is lacking. Dr. Wilkoff pointed out that more evidence is needed in areas such as indications for CRT implantation, how to measure success, the definition of “nonresponse,” and the role of comorbidities such as AF.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.