

Summary
This article presents the current management of patients with chronic coronary artery disease (CAD) by highlighting key concepts from the 2012 Guidelines for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease [Fihn SD et al. J Am Coll Cardiol 2012]. The guidelines include detailed algorithms for diagnosis, risk assessment, guideline-directed medical therapy (GDMT), and revascularization to improve symptoms. The discussion continues with suggestions on how the 2011 Performance Measures for Adults With Coronary Artery Disease and Hypertension [Drozda J Jr et al. J Am Coll Cardiol 2011] could provide some insight into the direction of the new guidelines.
- Cardiology Guidelines
- Coronary Artery Disease
- Cardiology & Cardiovascular Medicine
- Cardiology Guidelines
- Coronary Artery Disease
- Exclusive Article - For home page
Stephan D. Fihn, MD, MPH, University of Washington, Seattle, Washington, USA, discussed the current management of patients with chronic coronary artery disease (CAD) by highlighting key concepts from the 2012 Guidelines for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease [Fihn SD et al. J Am Coll Cardiol 2012]. The guidelines include detailed algorithms for diagnosis, risk assessment, guideline-directed medical therapy (GDMT), and revascularization to improve symptoms.
The key concepts from the guideline include the following:
-
▪ Management of stable ischemic heart disease (SIHD) should be based on strong scientific evidence and patient preference.
-
▪ Patients presenting with angina should be categorized as stable versus unstable. Those at moderate or high risk should be treated emergently for acute coronary syndrome.
-
▪ A standard exercise test is the first choice to diagnose IHD for patients with an interpretable electrocardiogram (ECG) and the ability to exercise, especially if the likelihood is intermediate (10% to 90%).
-
▪ Those who have an uninterpretable ECG and are able to exercise should undergo an exercise stress test with nuclear myocardial perfusion imaging (MPI) or echocardiography, particularly if likelihood of IHD is >10%.
-
» If unable to exercise, MPI or echocardiography with pharmacologic stress is recommended.
-
-
▪ Patients diagnosed with SIHD should undergo assessment of risk for death or complications.
-
▪ For patients with an interpretable ECG and who the ability to exercise, a standard exercise test is also the preferred choice for risk assessment.
-
» Those who have an uninterpretable ECG and are able to exercise should undergo an exercise stress with nuclear MPI or echocardiography, while for those patients unable to exercise, a nuclear MPI or echocardiography with pharmacologic stress is recommended.
-
-
▪ Patients with SIHD should generally receive a “package” of GDMT that includes lifestyle interventions and medications shown to improve outcomes. This includes the following (as appropriate):
-
» Diet, weight loss, and regular physical activity;
-
» if a smoker, smoking cessation;
-
» aspirin 75 to 162 mg daily;
-
» a statin medication in moderate dosage;
-
» if hypertensive, antihypertensive medication to achieve a blood pressure (BP) <140/90 mm Hg; and
-
» if diabetic, appropriate glycemic control.
-
-
▪ Patients with angina should receive sublingual nitroglycerin and a β-blocker. When these are not tolerated or are ineffective, a calcium-channel blocker or long-acting nitrate may be substituted or added.
-
▪ Coronary arteriography should be considered for patients with SIHD whose clinical characteristics and results of noninvasive testing indicate a high likelihood of severe IHD and when the benefits are deemed to exceed risk.
-
▪ The relatively small proportion of patients who have “high-risk” anatomy (eg, >50% stenosis of the left main coronary artery), revascularization with coronary artery bypass grafting should be considered to potentially improve survival. Most data showing improved survival with surgery compared with medical therapy are several decades old and based on surgical techniques and medical therapies that have advanced considerably. There are no conclusive data demonstrating improved survival following percutaneous coronary intervention.
-
▪ Most patients should have a trial of GDMT before considering revascularization to improve symptoms. Deferring revascularization is not associated with worse outcomes.
-
▪ Prior to revascularization to improve symptoms, coronary anatomy should be correlated with functional studies to ensure lesions responsible for symptoms are targeted.
-
▪ Patients with SIHD should be carefully followed to monitor progression of disease, complications, and adherence (Table 1).
-
» Exercise and imaging studies should generally be repeated only when there is a change in clinical status (not annually).
The Scientific Statement from the American Heart Association (AHA), the American College of Cardiology Foundation (ACCF), and the American Society of Hypertension (ASH) on the Treatment of Hypertension in the Prevention and Management of Ischemic Heart Disease is expected for publication later this year (2013). A prepublication embargo prevented discussion at this year's annual ACC meeting. Suzanne Oparil, MD, University of Alabama at Birmingham, Birmingham, Alabama, USA, suggested that the 2011 Performance Measures for Adults With Coronary Artery Disease and Hypertension [Drozda J Jr et al. J Am Coll Cardiol 2011] could provide some insight into the direction of the new guidelines. Specifically, she noted that the 2011 measures go beyond targeting established BP goals. The goal of antihypertensive treatment in patients with CAD or at high cardiovascular disease (CVD) risk was defined as <140/90 mm Hg. The rationale behind this change from a prior goal of <130/80 mm Hg was that some clinical trials in which specific antihypertensive drug therapies were given to individuals with CAD or high CVD risk who had BP <140/90 mm Hg showed benefit, but others had negative or equivocal findings. This heterogeneity in the published literature was used to justify a less strict (<140/90 mm Hg) BP goal in the performance measures. While the authors acknowledge that lower BP targets may be appropriate for some patients with CAD or other conditions, it is unclear how such patients could be reliably identified for purposes of performance measurement. In Dr. Oparil's opinion, the strongest evidence in support of the concept that “lower is not better” is the ACCORD trial, which showed no benefit from intensive (<120 mm Hg) versus standard (<140 mm Hg) BP control in terms of fatal and nonfatal major CV events in patients with type 2 diabetes at high risk for CV events [ACCORD Study Group. N Engl J Med 2010]. Subanalyses and post hoc reports from the INVEST [Cooper-DeHoff RM et al. JAMA 2010] and ONTARGET trials [Mancia G et al. Circulation 2011] provide similar findings. Although the Systolic Blood Pressure Intervention Trial [SPRINT; NCT01206062] will likely not end until 2016 or later. Dr. Oparil said the results are highly anticipated as it is designed to assess the effects of intensive BP lowering (<120 vs <140 mm Hg) on major CV events in patients without diabetes but with CVD risk factors, including chronic kidney disease, clinical CVD (excluding stroke), and age >75 years.
Noninvasive Testing in Known SIHD
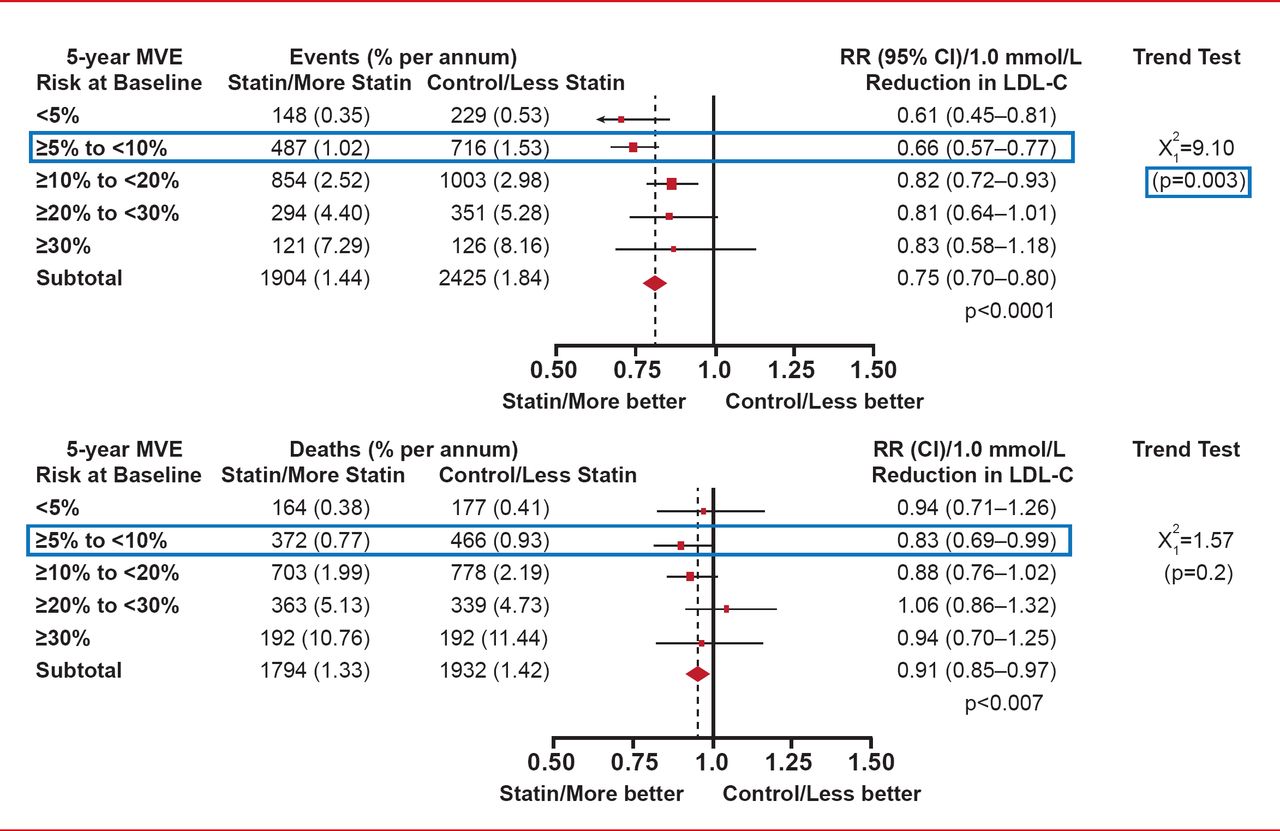
As with the 8th report on the Joint National Commitee on Prevention, Detection, Evaluation and Treatment of Hypertension (JNC8), the Guidelines for the Management of High Blood Pressure in Adults – JNC 2013, the new guidelines for treating lipids in patients at risk for CVD (Adult Treatment Panel; ATP IV) are also still in development. In lieu of a discussion of the guidelines, Jennifer G. Robinson, MD, MPH, University of Iowa, Iowa City, Iowa, USA, discussed new evidence published since the committee completed their work and some of the evidence considered in the development of the guidelines. Of recent interest are the results of a meta-analysis of 27 primary and secondary prevention trials (n=134,537 participants) that evaluated the effects of using statins to lower low-density lipoprotein cholesterol (LDL-C) in individuals at low risk of CVD [Cholesterol Treatment Trialists' Collaborators. Lancet 2012]. A key finding of the study was that for individuals with a 5-year risk of major vascular events of <10% (a population of patients not typically considered suitable for statin therapy), each 1-mmol/L reduction in LDL-C produced an absolute reduction in major vascular events of approximately 1.1%. In particular, those patients without a history of vascular disease and a 5% to <10% 5-year major CVD risk experienced a significant reduction (34%; p=0.003 for trend) in the relative risk of major CVD and a borderline significant 17% reduction in total mortality compared with those in the higher risk groups (Figure 1).
The AHA recently issued a statement on triglycerides and CVD [Miller M et al. Circulation 2011]. Dr. Robinson briefly summarized that statement noting that the focus in patients with triglyceride levels <500 mg/dL should be on decreasing the risk for CVD through improved diet, increased physical activity, and weight loss, and by getting the patient on a statin. These patients should also be assessed for diabetes. Treatment is the same for patients whose triglyceride level is >500 mg/dL, but with the additional focus of preventing pancreatitis.
This session offered some early insights into the long-awaited and eagerly anticipated release of the JNC-8 and ATP IV guidelines.

Reduction in Major CVD Risk Among Primary Prevention Patients With a 5% to 10% 5-Year Major CVD Risk per 1 mmol Reduction in LDL-C With a Statin
CVD=cardiovascular disease; LDL-C=low-density lipoprotein cholesterol; MVE=major vascular events.
Adapted from Mihaylova B et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. The Lancet Aug 2012;380(9841):581–590.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.