

Summary
Another guideline-focused session brought together several experts to discuss the 2013 American College of Cardiology Foundation /American Heart Association Guidelines for the management of ST-elevation myocardial infarction [O'Gara PT et al. J Am Coll Cardiol 2013].
- Myocardial Infarction
- Cardiology Guidelines
- Thrombotic Disorders
- Myocardial Infarction
- Cardiology Guidelines
- Thrombotic Disorders
- Cardiology
Another guideline-focused session brought together several experts to discuss the 2013 American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) Guidelines for the management of ST-elevation myocardial infarction (STEMI) [O'Gara PT et al. J Am Coll Cardiol 2013].
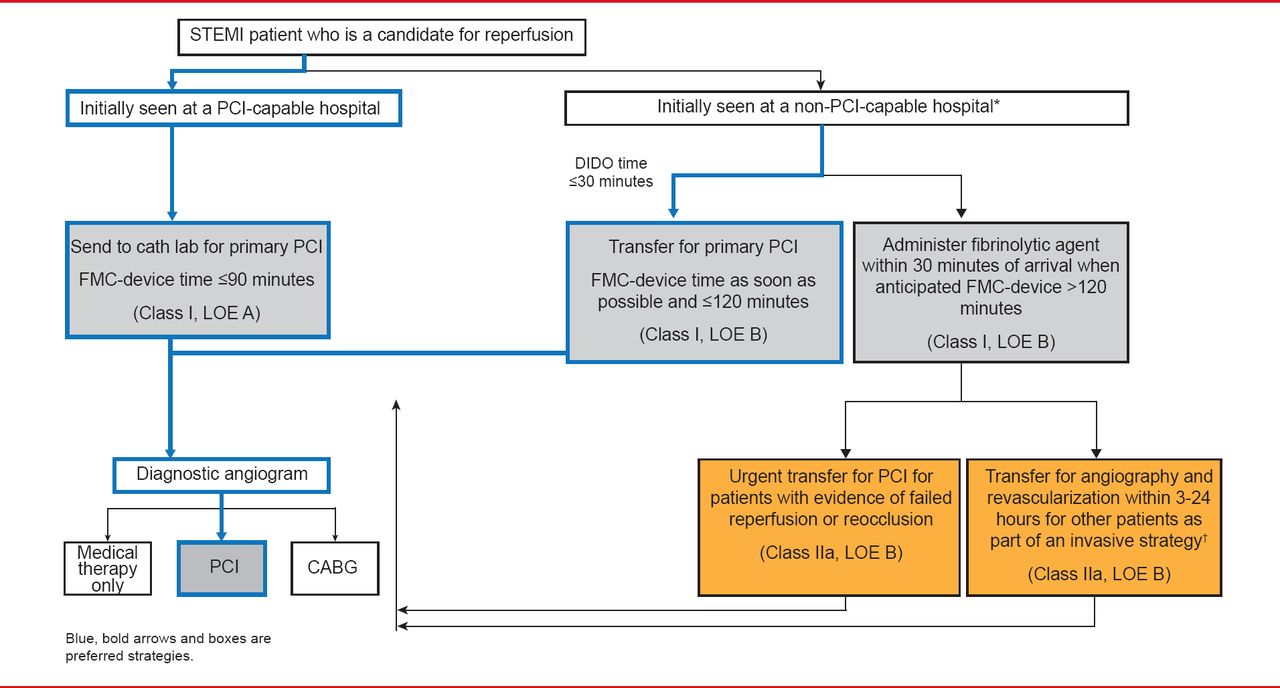
Patrick T. O'Gara, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, spoke about some of the changes in the new guidelines and some important recommendations that have been reaffirmed. In Dr. O'Gara's opinion, the key take-home messages from these guidelines are in the algorithm for triage and treatment for patients with suspected STEMI (Figure 1). Using this algorithm,
-
▪ STEMI patients who are candidates for reperfusion who are seen at a percutaneous coronary intervention (PCI)-capable hospital should be sent to the catheterization laboratory for primary PCI within 90 minutes of first medical contact (FMC; Class I, Level of Evidence [LOE] A).
-
▪ Patients initially seen at a non-PCI-capable hospital should be transferred to a primary PCI-capable facility within 30 minutes provided that the FMC was ≤120 minutes. When this is not possible, full-dose fibrinolytic therapy should be administered within 30 minutes of arrival at the non-PCI capable facility (Class I, LOE B).
-
▪ In a departure from previous guidelines, the committee now recommends that it is reasonable to transfer patients to a PCI-capable facility after fibrinolytic therapy has been administered regardless of whether the fibrinolytic therapy was successful (Class IIa, LOE B).

Reperfusion Therapy for Patients With STEMI
CABG=coronary artery bypass grafting; DIDO=door-in to door-out; FMC=first medical contact; LOE=level of evidence; PCI=percutaneous coronary intervention; STEMI=ST-elevation myocardial infarction.
†Angiography and revascularization should not be performed within the first 2 to 3 hours after administration of fibrinolytic therapy.
Reproduced from O'Gara PT et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. Journal of the American College of Cardiology 2013;61(4):e78–104. With permission from Elsevier.
Other changes in the new guidelines include the recommendation that emergency medical service (EMS) personnel perform a 12-lead electrocardiogram (ECG) at the site of FMC (Class I, LOE B). There is a strong recommendation against PCI of a noninfarct artery at the time of primary PCI in patients without hemodynamic compromise (Class III: Harm LOE B). However, PCI may be appropriate later in patients with spontaneous symptoms of myocardial ischemia (Class I, LOE C) and in patients with intermediate- or high-risk findings on noninvasive testing (Class IIa, LOE B).
The guideline also recommends institution of therapeutic hypothermia as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest due to ventricular fibrillation or pulseless ventricular tachycardia. Patients who are resuscitated after out-of-hospital cardiac arrest whose initial ECG shows ST segment elevation should also undergo coronary angiography and primary PCI (both Class I, LOE B).
Low-dose aspirin (81 mg QD) is now the preferred maintenance dose to support reperfusion with PCI (Class IIa, LOE B); prasugrel should not be used in patients with STEMI with a history of stroke (Class III: Harm LOE B). Given the current uncertainty about its routine use [Thiele H et al. N Engl J Med 2012], the recommendation for the use of intra-aortic balloon pump counterpulsation in patients with cardiogenic shock after STEMI who do not quickly stabilize with pharmacological therapy has been downgraded to Class IIa, LOE B.
All patients with STEMI should receive high-intensity statin therapy (Class I, LOE B), unless there is a clear contraindication. Anticoagulant therapy with a vitamin K antagonist should be provided to patients with STEMI and atrial fibrillation with CHADS2 score ≥2, mechanical heart valves, venous thromboembolism, or hypercoagulable disorder. The duration of triple-antithrombotic therapy with a vitamin K antagonist, aspirin, and a P2Y12 receptor inhibitor should be minimized to limit the risk of bleeding (both Class I, LOE C).
PCI is clearly superior to fibrinolytics when performed in a timely manner by experienced operators, said Ivan Rokos, MD, David Geffen School of Medicine at University of California, Los Angeles, Los Angeles, California, USA. Under the new guidelines, all communities should create and maintain a regional system of STEMI care that includes assessment and continuous quality improvement of EMS and hospital-based activities. The guidelines suggest the use of programs such as the AHA's Mission: Lifeline and the ACC's Door-to-Balloon (D2B): An Alliance for Quality to facilitate performance (Class I, LOE B).
The goal of a STEMI system is to route patients to a PCI-capable hospital within guideline benchmarks, regardless of how or where they initially enter the system. Two new programs are making the implementation and management of these systems more efficient and effective. As of 2012, standardized high-quality regional reports are available from the ACC/AHA's Acute Coronary Treatment and Intervention Outcomes Network registry-Get With the Guidelines (ACTION-GWTG) that show the performance of all ACTION-GWTG registry hospitals in a particular community as well as outcome measures (eg, risk-adjusted mortality) that can be used for benchmarking and quality improvement. In addition, Geospatial Information Systems maps available through the Mission: Lifeline website are increasingly making it possible to map regions and states to show the location of PCI- and non-PCI-capable hospitals and their referral hospitals, thus providing a mechanism to manage the flow of patients [Rokos I et al. Crit Pathw Cardiol 2013].
PCI is clearly superior to fibrinolytics when performed in a timely manner by experienced operators.
To-date, the existing STEMI systems have focused on quality, but Dr. Rokos believes that it is time to change the focus to value—value that can be increased through faster reperfusion, and lower morbidity and hospitalization cost. He proposed creating Time-Critical Accountable Care Organizations that cover entire states or regions of >1 million people [Rokos IC. Circ Cardiovasc Qual Outcomes 2011]. These organizations would operate much like their primary-care counterparts but they would focus on hyper-acute situations like STEMI, stroke, and resuscitation. Importantly, they would operate under a regional pay-for-performance system in that all hospitals in the system would benefit when goals are met (vs just the larger organizations).
Stephen D. Wiviott, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed the use of adjunctive pharmacologic therapy in the setting of PCI. Although there are several options for anticoagulation with primary PCI, clinical data and the guidelines favor the use of bivalirudin (Class I, LOE B) as it has similar efficacy to heparin plus a glycoprotein IIb/IIIa inhibitor with improved safety and ultimately improved survival [Stone G et al. N Engl J Med 2008]. However, the very early occurrence of stent thrombosis in the HORIZONS AMI study underscored the need for early and potent antiplatelet therapy in the setting of primary PCI.
As to the best choice of antiplatelet, the guidelines offer providers the choice of using clopidogrel, prasugrel, or ticagrelor. Compared with clopidogrel, both prasugrel and ticagrelor have more rapid onset and offer more potent and consistent antiplatelet effect but at the expense of higher bleeding complications. [Montalescot G et al. Lancet 2009; Steg PG et al. Circulation 2010]. With these new guidelines, clinicians have a comprehensive summary of the data driven approaches to pre-, peri-, and post-hospital care of patients with STEMI that have been demonstrated to lead to decreased patient morbidity and mortality.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.