

Summary
Fibrinolytic therapy coupled with timely coronary angiography results in effective reperfusion in patients with ST-segment elevation myocardial infarction who cannot undergo primary percutaneous coronary intervention within 1 hour of presentation, according to the results of the Strategic Reperfusion (With Tenecteplase and Antithrombotic Treatment) Early After Myocardial Infarction trial [STREAM; Armstrong PW et al. N Engl J Med 2013].
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Myocardial Infarction
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Myocardial Infarction
Fibrinolytic therapy coupled with timely coronary angiography results in effective reperfusion in patients with ST-segment elevation myocardial infarction (STEMI) who cannot undergo primary percutaneous coronary intervention (PCI) within 1 hour of presentation, said Frans Van de Werf, MD, PhD, University of Leuven, Leuven, Belgium, who presented the results of the Strategic Reperfusion (With Tenecteplase and Antithrombotic Treatment) Early After Myocardial Infarction trial [STREAM; Armstrong PW et al. N Engl J Med 2013].
Although prompt delivery of primary PCI is the preferred strategy to treat patients with acute STEMI, delays in performing PCI are common when patients present to emergency medical services or hospitals without the capability for catheterization. The delay in reperfusion that results from long transfer to a hospital for primary PCI increases the rates of morbidity and mortality.
In STREAM, patients with STEMI (≥2 mm ST elevation in 2 contiguous leads) who presented within 3 hours of symptom onset and who could not undergo primary PCI within 1 hour of first medical contact were randomized to 1 of 2 strategies: 1) early fibrinolysis followed by coronary angiography in 6 to 24 hours or rescue PCI, if needed, or 2) standard primary PCI. Patients from 99 sites in 15 countries were included in this trial.
In the early fibrinolysis group, patients received a weight-based bolus of tenecteplase along with aspirin, clopidogrel, and enoxaparin in the ambulance or emergency department. Rescue intervention was performed if there was <50% ST-segment resolution in the single lead of an electrocardiogram or clinical evidence of failed reperfusion within 90 minutes after fibrinolytic therapy. In the primary PCI group patients received antiplatelet and antithrombin treatment according to local guidelines, and underwent standard primary PCI.
The trial was designed as a proof-of-concept study where all statistical tests were of an exploratory nature. The primary endpoint was a composite of death, shock, congestive heart failure, or reinfarction at 30 days [Armstrong PW et al. N Engl J Med 2013].
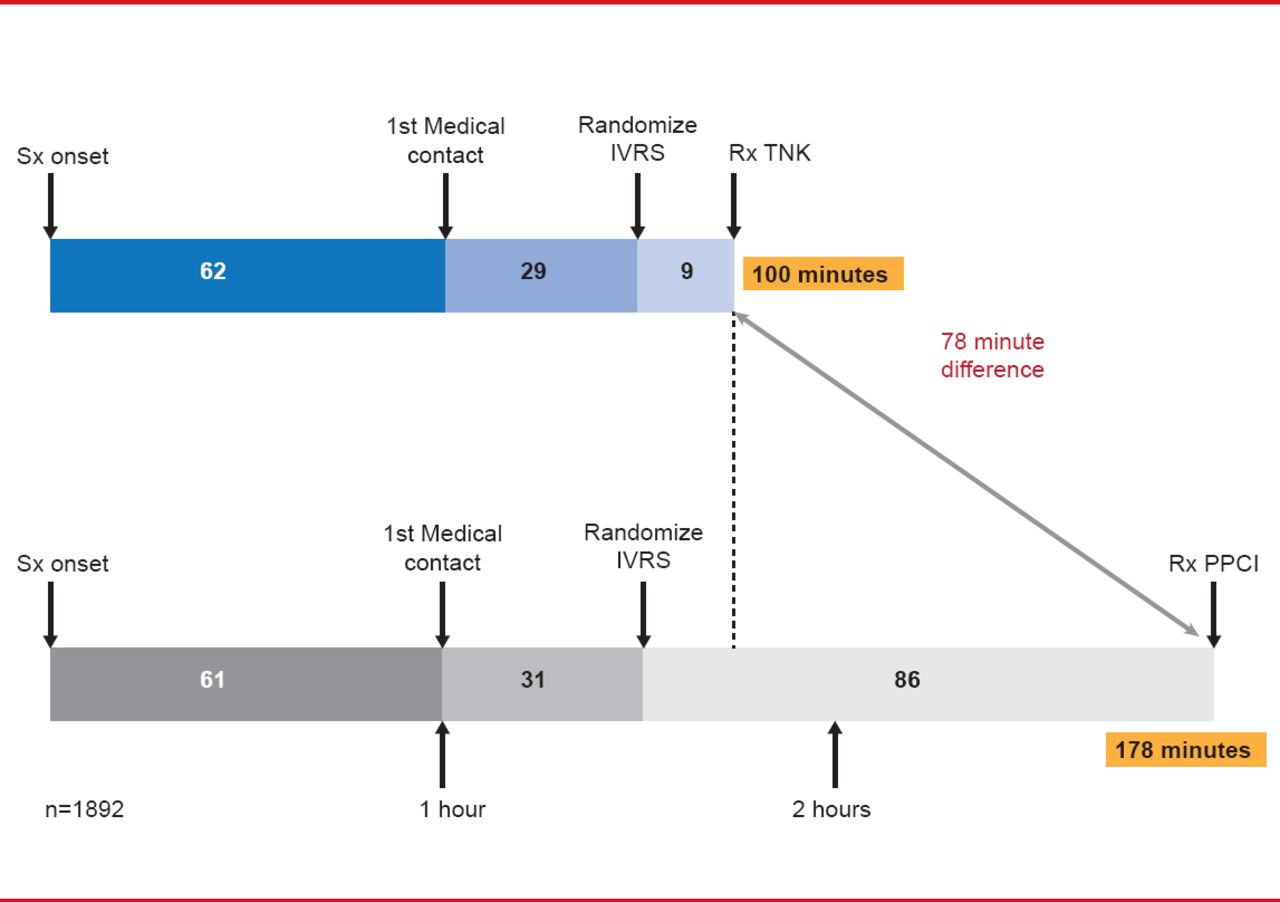
After 20% of the planned recruitment into the study, the bolus dose of tenecteplase was halved in patients aged ≥75 years to reduce the risk of intracranial bleeding. A total of 1892 patients were randomized. The median time from symptom onset to the start of reperfusion therapy was 100 minutes in patients randomized to the early fibrinolysis group versus 178 minutes in the primary PCI group (Figure 1).

Median Time to Treatment: Early Fibrinolysis Versus Primary PCI
IVRS=interactive voice response system; PPCI=primary percutaneous coronary intervention; TNK=tenecteplase.
Reproduced with permission from F Van de Werf, MD, PhD.
In the 36% of the patients who required rescue or urgent PCI the median time to PCI following bolus tenecteplase was 2.2 hours. In the remaining 64% a nonurgent angiography was performed after a median of 17 hours
Patients assigned to early fibrinolysis were more likely to have Thrombolysis in Myocardial Infarction (TIMI)-3 blood flow prior to PCI compared with the primary PCI group (58.5% vs 20.7%; p<0.001) but there was no significant difference in TIMI-3 blood flow after PCI (91.1 % vs 92.3%; p=0.41). Coronary artery bypass graft surgery was performed about twice as often in the early fibrinolysis versus the primary PCI group (4.7% vs 2.1%; p=0.002).
STREAM suggests that a strategy involving early fibrinolysis in appropriate patients on a background of contemporary antithrombotic therapy may be beneficial in patients with STEMI who present within 3 hours of symptom onset and who cannot undergo primary PCI within 1 hour of first medical contact. An important implication of STREAM is the key role of prehospital systems capable of early diagnosis, therapy, and triage at the first point of care. In addition, STREAM underscores the importance of efforts to improve the availability of primary PCI for patients presenting with STEMI.
Science Advisor's note: As specified in the methods the statistical testing was considered exploratory and therefore these findings should be considered hypothesis-generating.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.