

Summary
A post hoc subanalysis of the Digitalis Investigation Group [DIG] trial found that digoxin reduces all-cause hospital admission at 30 days in older ambulatory patients with chronic systolic heart failure (HF) [Bourge RC. Am J Med 2013]. Reduction in hospital readmissions is of particular interest in the United States due to related financial penalties levied by the Center for Medicare and Medicaid Services from October 2012 for older patients with HF.
- Heart Failure
- Cardiology Clinical Trials
- Heart Failure
- Cardiology Clinical Trials
- Cardiology
A post hoc subanalysis of the Digitalis Investigation Group trial found that digoxin reduces all-cause hospital admission at 30 days in older ambulatory patients with chronic systolic heart failure (HF) [Bourge RC. Am J Med 2013]. Reduction in hospital readmissions is of particular interest in the United States due to related financial penalties levied by the Center for Medicare and Medicaid Services (CMS) from October 2012 for older patients with HF.
The objective of the post hoc analysis by Ali Ahmed, MD, MPH, University of Alabama, Birmingham, Alabama, USA, and colleagues, was to examine the effect of digoxin on 30-day all-cause hospital admission in a subgroup of older, potentially Medicare-eligible, adults with HF and reduced ejection fraction from the main DIG trial which randomized 6800 ambulatory patients with chronic HF to either digoxin or placebo on a background of standard therapy from 1991 through 1993 [DIG Investigators. N Engl J Med 1997].
The presented analysis included a subset of 3405 patients aged ≥65 years with chronic HF (ejection fraction ≤45%) in normal sinus rhythm from the United States and Canada. They had a mean age of 72 (±5) years, 25% were women, 76% had a primary etiology of ischemic heart failure, 61% had chronic kidney disease, and 11% were nonwhite. Angiotensin-converting enzyme inhibitors were used at baseline in 94% and diuretics were used in 82%. The proportion on β-blockers was not collected.
In the subgroup of interest, 1712 were randomized to digoxin and 1693 to placebo. Overall, baseline characteristics between groups were similar except for a slightly lower body mass index among those assigned to digoxin (p=0.04).
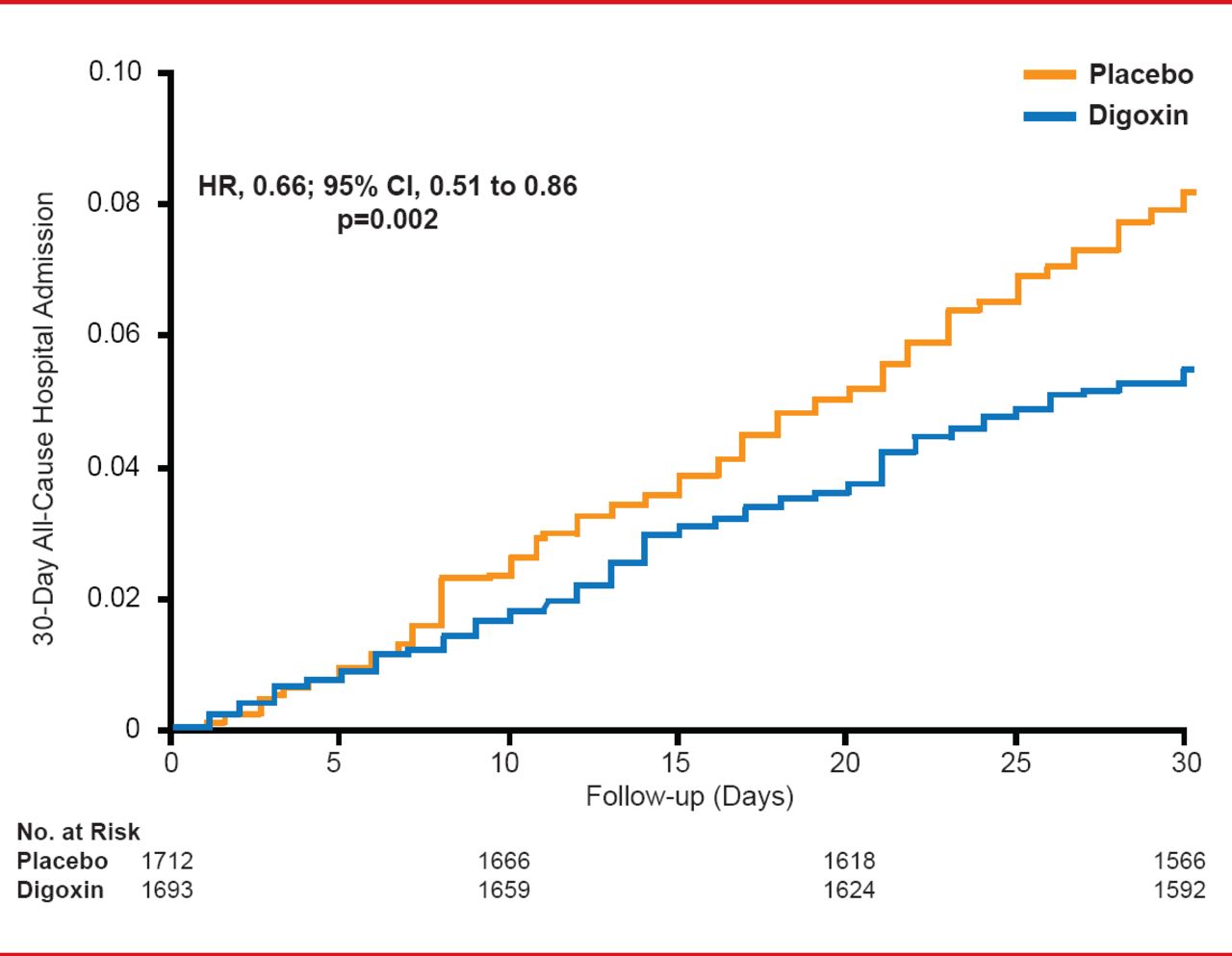
In the 30 days after randomization, the all-cause hospital admission rate was significantly lower in the digoxin- versus placebo-treated group (5.4% vs 8.1%, respectively; HR, 0.66; 95% CI, 0.51 to 0.86; p=0.002; Figure 1). Over the same time period, digoxin reduced both the absolute (−2.7%) and relative (−34%) risks of all-cause hospital admission.

30-Day All-Cause Hospital Admissions With Digoxin Versus Placebo
Reproduced with permission from A Ahmed, MD, MPH.
The reduction in all-cause hospital admissions with digoxin persisted through 60 days (HR, 0.76; 95% CI, 0.63 to 0.91; p=0.003) and 90 days (HR, 0.75; 95% CI, 0.63 to 0.88; p<0.001) post randomization. This suggests that the early benefit of digoxin was not achieved at the cost of harm at a later time.
In the 30 days following randomization, digoxin significantly reduced the risk of hospital admission due to cardiovascular causes by 47% (HR, 0.53; 95% CI, 0.38 to 0.72; p<0.001) and due to worsening HF by 60% (HR, 0.40; 95% CI, 0.26 to 0.62; p<0.001). Differences between 30-day mortality outcomes for all-cause and cardiovascular mortality were not significant between the digoxin and placebo groups. A favorable trend toward less frequent progression of HF (HR, 0.22; 95% CI, 0.05 to 1.04; p=0.056) was observed with digoxin.
Since these results were derived from post hoc subgroup analyses, the findings should be considered hypothesis-generating that require confirmation in prospective studies. Clinicians should be cautious about generalizing these results to patients in clinical practice, in part because the study was conducted in the early 1990s when current background therapies were either not standard-of-care (eg, β-blockers, spironolactone) or unavailable (eg, angiotensin receptor blockers).
If these findings can be replicated in current older HF patients on guideline recommended background therapy, digoxin may be a low-cost option to reduce 30-day all-cause readmissions and avoid penalties imposed by CMS.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.