

Summary
While the 2013 Joint National Committee Guidelines for the Management of High Blood Pressure in adults still under revision and not available for discussion, this article discusses new and important recommendations from the Canadian Hypertension Education Program [Daskalopoulou SS et al. Can J Cardiol 2012].
- Hypertensive Disease
- Cardiology & Cardiovascular Medicine
- Hypertensive Disease
With the 2013 Joint National Committee Guidelines for the Management of High Blood Pressure (BP) in adults still under revision and not available for discussion, Suzanne Oparil, MD, University of Alabama at Birmingham, Birmingham, Alabama, USA, discussed new and important recommendations from the Canadian Hypertension Education Program (CHEP) [Daskalopoulou SS et al. Can J Cardiol 2012].
In the last few years, out-of-office (home) BP measurement has assumed a more prominent role in the diagnosis and follow-up of hypertensive patients, in part because it may help to identify “white coat” or “masked” hypertension. Differentiation is important because those with masked hypertension have a higher rate of cardiovascular events compared with patients who are normotensive or have white coat hypertension. Previously, patients who were found to have normal BP at home (ie, <135/85 mm Hg) but elevated readings in the office were recommended for 24-hour ambulatory monitoring to confirm white coat hypertension. The Task Force has now added repeat home BP monitoring as another method to confirm white coat hypertension in such patients.
The Task Force also made an important modification to the management recommendations for patients with hypertension associated with nondiabetic chronic kidney disease. After a comprehensive reassessment of the evidence examining BP targets in this patient population, it concluded that there was insufficient evidence to support a target of 130/80 mm Hg. Therefore, the target BP in this patient population was changed to <140/90 mm Hg, similar to the general population.
The summary of evidence from CHEP for patients with diabetes and hypertension suggest lowering systolic BP to <140 mm Hg to reduce all-cause mortality and stroke, with systolic BPs <135–130 mm Hg appearing to confer significant additional benefits with respect to stroke. Although the risk of serious adverse events increases with BPs <140 mm Hg, the absolute number of these risk events is low, and therefore, the <130/80 mm Hg BP target in patients with diabetes remained unchanged in the current CHEP recommendations.
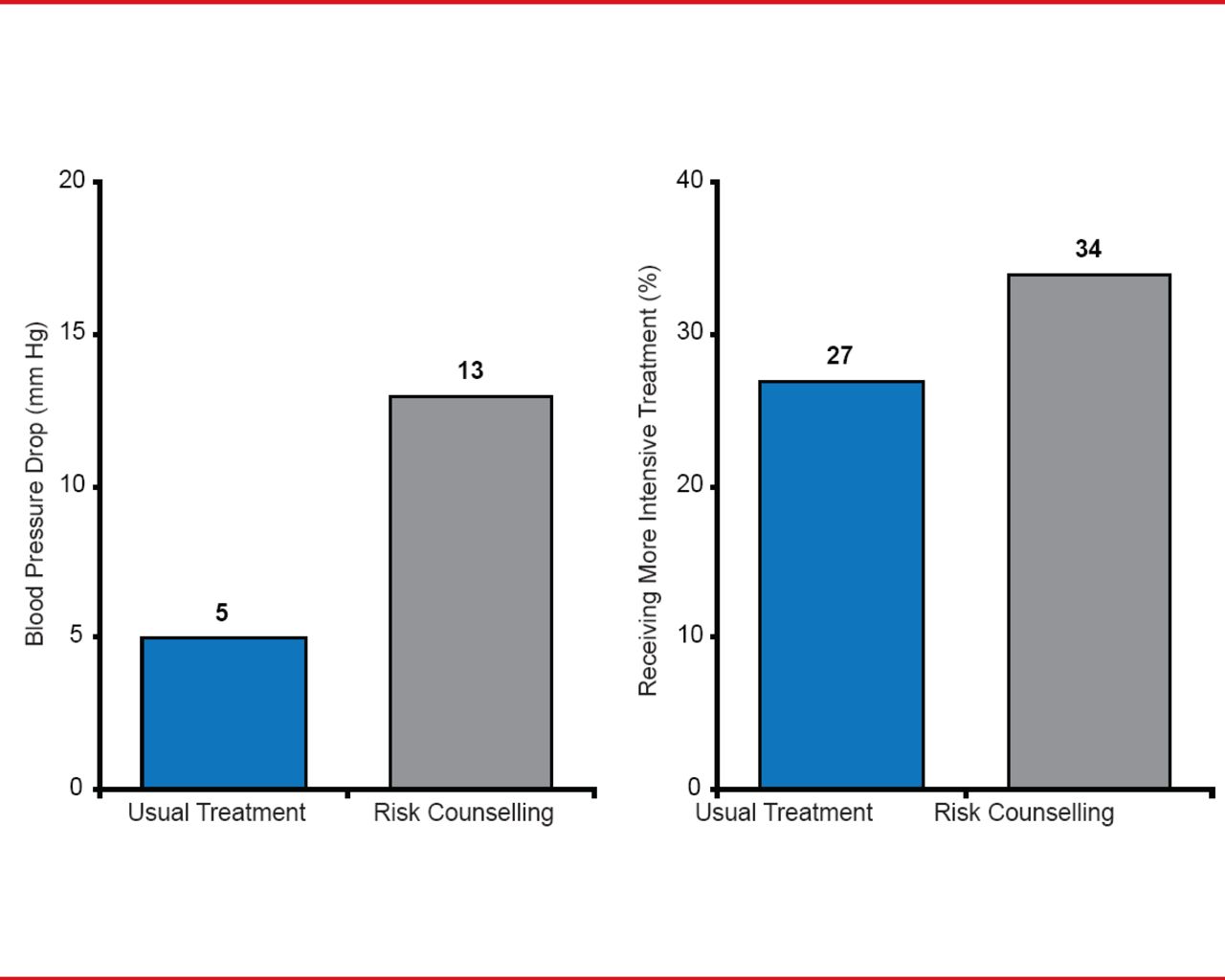
Monotherapy is often not enough [Cushman WC et al. J Clin Hypertens (Greenwich) 2002], especially for patients with diabetes, and therefore, many hypertensive patients now receive ≥2 antihypertensive agents. According to the Task Force, using single pill combinations may help to achieve BP control by improving medication compliance. Another way to improve patient compliance with BP treatment is to start an ongoing counseling to discuss and assess coronary risk (Figure 1) [Grover SA et al. J Gen Intern Med 2009].

Impact of Discussing Coronary Risk With Hypertensive Patients
The American Diabetes Association's (ADA) 2013 edition of Standards of Medical Care in Diabetes recommends that individuals with diabetes and hypertension be treated to a systolic BP goal of <140 mm Hg consistent with the CHEP guidelines [ADA Diabetes Care 2013]. In contrast, however, they note that some lower targets for specific patients and for diastolic BP including a systolic BP target of <130 mm Hg may for certain individuals (eg, younger patients) if it can be achieved without unnecessary treatment burden and target diastolic BP for diabetic patients of <80 mm Hg. Patients with BP >120/80 mm Hg should be persuaded to make lifestyle changes, while those with BP ≥140/80 mm Hg should begin treatment with ≥1 pharmacological agents (either an angiotensin-converting enzyme inhibitor or angiotensin II receptor blocker) plus lifestyle therapy to achieve BP goals. Finally, for pregnant patient with diabetes and chronic hypertension, the ADA suggests BP target goals of 110/65 to 129/79 mm Hg in the interest of long-term maternal health and to minimize impaired fetal growth.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.