

Summary
Data from the 30-Day Cardiac Event Monitor Belt for Recording Atrial Fibrillation After a Cerebral Ischemic Event trial [EMBRACE; NCT00846924] showed that prolonged continuous cardiac monitoring to detect poststroke paroxysmal atrial fibrillation in patients with unexplained strokes is feasible, more effective than standard approaches, and leads to clinically meaningful changes in patient management.
- Nursing
- Arrhythmias
- Cerebrovascular Disease Clinical Trials
- Nursing
- Arrhythmias
- Cerebrovascular Disease
- Neurology Clinical Trials
- Neurology
Data from the 30-Day Cardiac Event Monitor Belt for Recording Atrial Fibrillation After a Cerebral Ischemic Event trial [EMBRACE; NCT00846924] presented by David J. Gladstone, MD, PhD, University of Toronto, Toronto, Ontario, Canada, showed that prolonged continuous cardiac monitoring to detect poststroke paroxysmal atrial fibrillation (AF) in patients with unexplained strokes is feasible, more effective than standard approaches, and leads to clinically meaningful changes in patient management.
Identification and treatment of AF can prevent second strokes; however, paroxysmal AF can be difficult to detect in patients with stroke or transient ischemic attack (TIA), and the most common screening method, 24-hour Holter monitoring, has a low sensitivity (∼5%) for detecting it post stroke. Small observational studies have suggested benefits of longer duration electrocardiogram (ECG) monitoring [Stahrenberg R et al. Stroke 2010; Sobocinski PD et al. Europace 2012; Flint AC et al. Stroke 2012]. The objective of the EMBRACE study, funded by the Canadian Stroke Network, was to determine the diagnostic yield of 30 days of home-based cardiac monitoring compared with repeat 24-hour Holter monitoring for detecting paroxysmal AF in patients with a recent diagnosis of cryptogenic ischemic stroke or TIA following a routine diagnostic stroke workup that included a negative Holter monitor. Secondary outcomes included monitoring adherence and anticoagulation status.
To be eligible for the study, patients had to be aged ≥55 years without previously documented AF, with a recent (≤6 months) diagnosis of a presumed embolic acute arterial ischemic stroke (confirmed by neuroimaging) or TIA of etiology (or suspected cardioembolic etiology but without proven AF). Subjects were required to have negative results on baseline tests that included ECG, Holter monitor, vascular imaging with computed tomography angiography or magnetic resonance angiography, and echocardiography. The primary study outcome was detection of ≥1 episode of AF or atrial flutter of ≥30 seconds within 90 days of randomization, confirmed by central adjudication. The study included 572 subjects (mean age, 73 years; ∼45% women). Sixty-three percent of the subjects had an ischemic stroke and 37% had a TIA. Baseline anticoagulant use was 5%. Over 90% of participants had a modified Rankin score of 0 to 2, indicating functional independence. Subjects were randomly assigned to repeat 24-hour Holter monitoring (n=285) or 30-day cardiac monitoring (n=287). In the 30-day group, subjects wore an event-triggered loop recorder (attached to a nonadhesive chest electrode belt) that was programmed to automatically record AF. They were instructed to wear this recorder for as much of the day as possible for up to 30 days or until AF was detected. The median number of days from the index event to randomization was about 70 (range, 45 to 103).
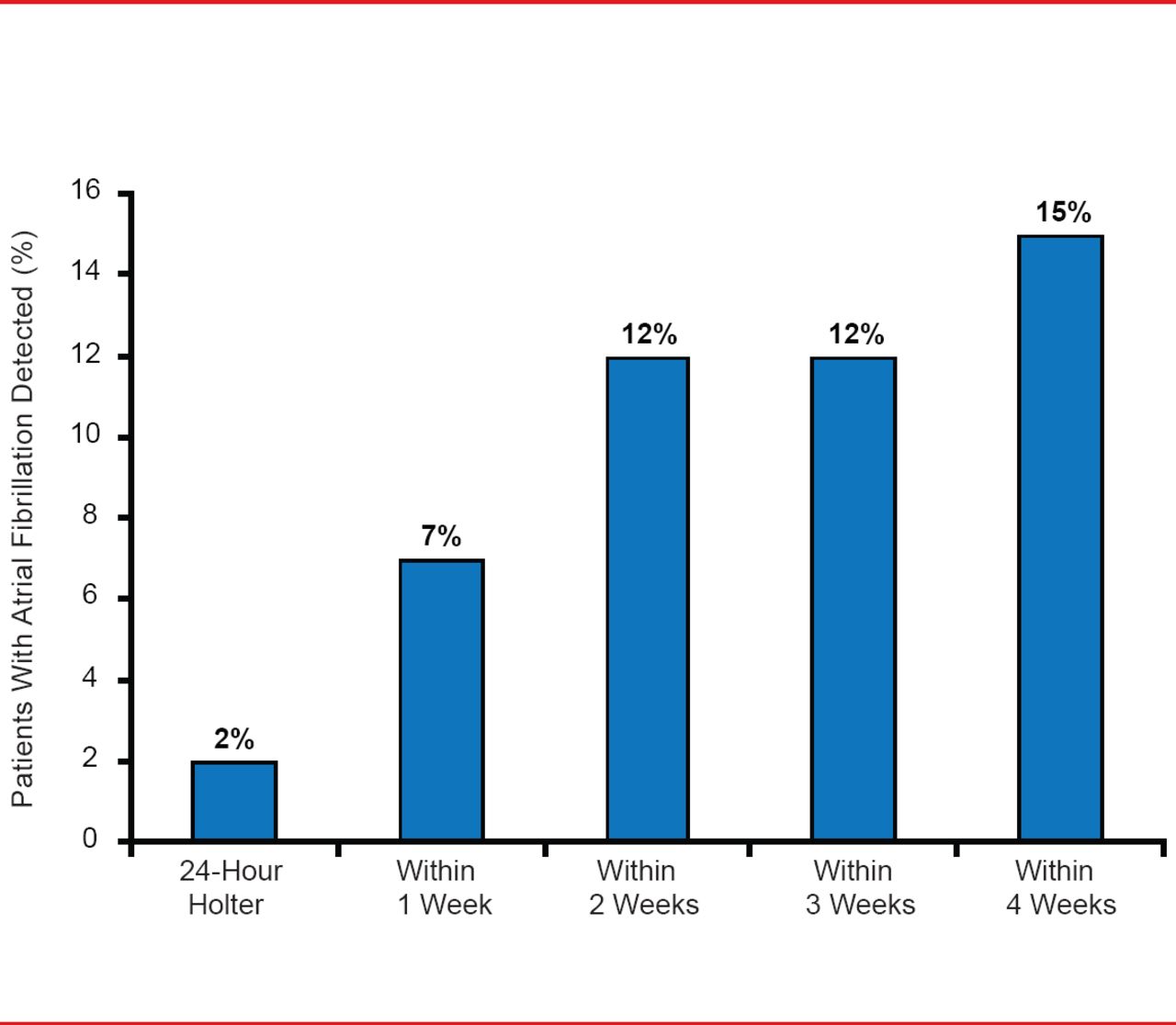
New AF was detected in significantly more patients in the 30-day group (16%) compared with the repeat Holter group (3%; p<0.001; Table 1). In the 30-day group, 82% of all participants wore their monitor for ≥3 weeks. Most AF events were captured within the first 2 weeks, with an incremental yield up to 30 days (Figure 1). Most patients with newly detected AF (72%) were placed on anticoagulants. Anticoagulant use increased by 90 days and was significantly greater in the 30-day group (18%) compared with the repeat Holter group (10%; p=0.01; Table 2).

Time to First Atrial Fibrillation Detection
Reproduced with permission from DJ Gladstone, MD, PhD.
Between-Group Comparison of Atrial Fibrillation Detection
The absolute difference in AF detection between the 30-day and the repeat Holter groups was 13%, which translates into a number needed to screen of 8 patients (to identify one additional patient with AF). The prevalence of AF detected was similar whether the index event was an ischemic stroke or TIA; the yield was highest among patients aged >75 years.
Anticoagulant Use
Dr. Gladstone noted that this study indicates that a substantial proportion of cryptogenic stroke or TIA patients have undiagnosed paroxysmal AF (1 in 6 patients aged ≥55 years; 1 in 5 patients aged >75 years), and it provides the strongest evidence to-date in support of prolonged cardiac monitoring in such patients. The findings of this trial have immediate implications for secondary stroke prevention.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.