

Summary
For a classification of systemic lupus erythematosus (SLE), patients must have at least one clinical and one immunologic criterion of the SLICC classification criteria, for a total of four, or must have biopsy-proven lupus nephritis. This article discusses prednisone for the treatment of SLE, the treatment of severe thrombocytopenia in SLE, severe cutaneous manifestations in patients with SLE, as well as subtypes of posterior reversible leukoencephalopathy syndrome, myelitis, and small-fiber neuropathies in SLE.
- Lupus
- Systemic Connective Tissue Disorders
- Rheumatology
- Lupus
- Systemic Connective Tissue Disorders
For a classification of systemic lupus erythematosus (SLE), patients must have at least one clinical and one immunologic criterion of the SLICC classification criteria, for a total of four, or must have biopsy-proven lupus nephritis. Clinical criteria include acute cutaneous lupus, chronic cutaneous lupus, oral ulcers, nonscarring alopecia, arthritis, serositus, neurologic lupus, proteinuria, and dytopenias [Petri M et al. Arthritis Rheum 2012]. Immunologic criteria include ANA, antids DNA, anti-Sm, antiphospholipid antibodies, low complement, and direct Coombs.
Michelle Petri, MD, MPH, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA, pointed out that prednisone is independently associated not just with non-life-threatening organ damage (cataracts, osteoporosis), but with cardiovascular events. [Madger LS, Petri M. Am J Epidem 2012; Thamer M et al. J Rheumatol 2009]. She emphasized that even low doses of prednisone >6 mg daily increase permanent organ damage. Most mild to moderate flares will respond to intramuscular triamcinolone or to a methylprednisolone “dose pack,” helping to avoid maintenance prednisone [Danowski A et al. J Rheumatol 2006]. Dr. Petri recommends administering hydroxychloroquine to all patients; it reduces flares [Canadian Hydroxychloroquine Study Group. N Engl J Med 1991] and thrombosis [Petri M. Scand J Rheumatol 1996; Pierangeli SS, Harris EN. Lupus 1996] by half, reduces organ damage [Fessler BJ et al. Arthritis Rheum 2005] and lipids [Petri M. Lupus 1996; Wallace DJ et al. Am J Med 1990], improves survival [Alarcon GS et al. Arthritis Rheum 2005; Ruiz-Irastorza G et al. Lupus 2005], prevents seizures [Hanly JG et al. Ann Rheum Dis 2012], and triples the response to mycophenolate [Kasitanon N et al. Lupus 2006] in severe lupus nephritis. Vitamin D is also a safe immunomodulator for patients with SLE [Petri M. Arthritis Rheum 2013].
TREATMENT OF THROMBOCYTOPENIA
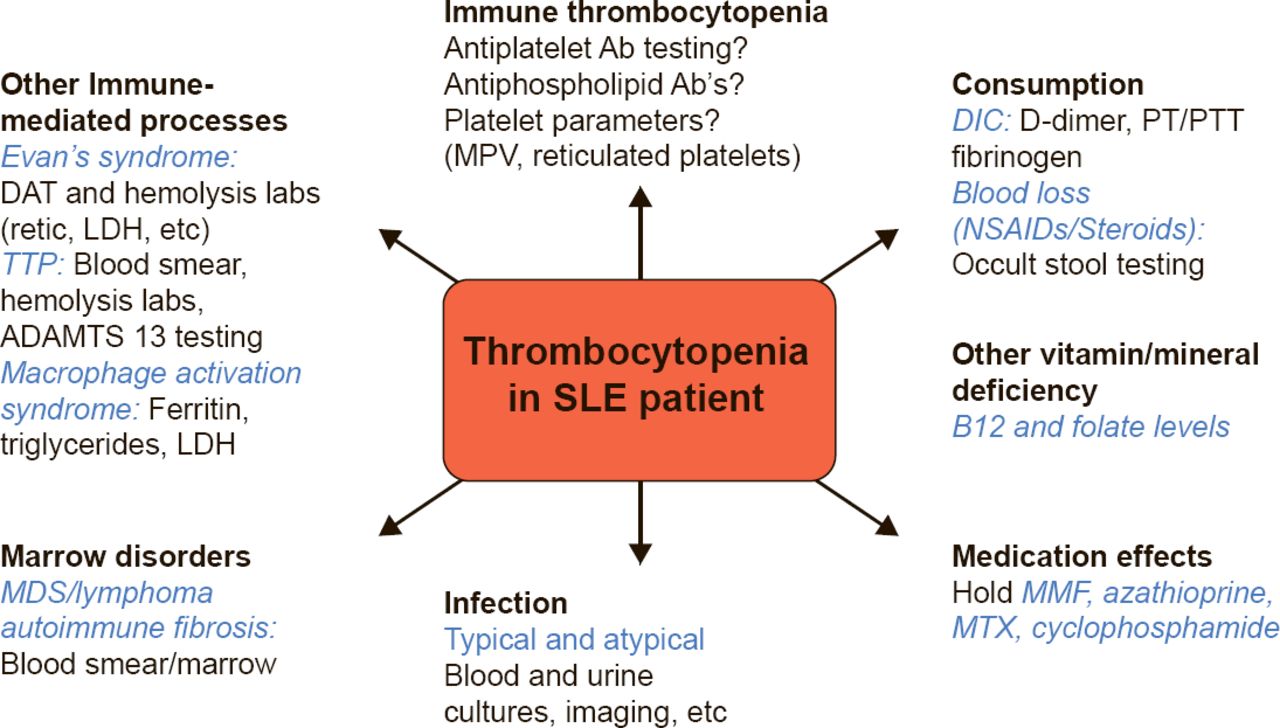
Brady L. Stein, MD, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA, discussed the treatment of severe thrombocytopenia in SLE. He agreed with Dr. Petri that long-term steroids have unacceptable adverse effects. Immune thrombocytopenia may result from impaired platelet production and/or increased platelet destruction mediated by autoantibodies, with subsequent splenic clearance. The differential diagnosis for thrombocytopenia in SLE is broad and a suggested diagnostic workup is summarized in Figure 1.

Thrombocytopenia in SLE: Differential Diagnosis and Workup
Ab=antibody; DAT=direct antiglobulin testing; DIC=disseminated intravascular coagulation;
LDH=lactate dehydrogenase; MDS=myelodysplastic syndrome; MMF=mycophenolate mofetil;
MPV=mean platelet volume; MTX=methotrexate; NSAIDs=nonsteroidal anti-inflammatory drugs; PT=prothrombin time; PTT=partial thromboplastin time; retic=reticulocyte count;
SLE=systemic lupus erythematosus; TTP=thrombotic thrombocytopenic purpura.
Reproduced with permission from M Petri, MD, MPH.
Patient factors affect the selection of therapy for thrombocytopenia. Younger patients may be better able to tolerate splenectomy. Comorbidities, cost, and SLE activity should also be considered. The typical threshold for therapy is a platelet count <20 to 30 × 109/L. For patients with antiphospholipid antibody syndrome who require anticoagulation, the threshold should be 50 × 109/L.
Splenectomy is an “old” treatment that yields high responses, although it has been analyzed in small numbers of patients with SLE [You YN. Ann Surgery 2004]. Another option is rituximab to suppress antibody production by B cells. Rituximab has been effective in primary idiopathic thrombocytopenic purpura (ITP), but this is an off-label use, may not be durable, and may be associated with adverse reactions in SLE patients [Gudbtrandsdottir S et al. Blood 2013; Jovancevic C et al. Lupus 2013; Neunert C et al. Blood 2011; Zaja F et al. Blood 2010; Godeau B et al. Blood 2008]. Other options are thrombopoietin agonists, like romiplostim [Kuter DJ et al. N Engl J Med 2010; Lancet 2008] and eltrombopag [Cheng G et al. Lancet 2011; Bussel JB et al. Lancet 2009], although results in SLE are anecdotal. These agents require long-term therapy and have potential side effects including thrombosis, a concern in SLE [Kuter DJ et al. Br J Haematol 2013; Saleh MN et al. Blood 2013].
TREATMENT OF NEUROLOGIC COMPLICATIONS
Julius Birnbaum, MD, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA, described subtypes of posterior reversible leukoencephalopathy syndrome (PRES), myelitis, and small-fiber neuropathies in SLE. PRES is associated with visual disturbances, encephalopathies, seizures, and headaches. Risk factors for PRES are similar in patients with or without SLE, and include hypertension, renal failure, immunosuppressant use, and thrombotic thrombocytopenic purpura (TTP). SLE is associated with many concomitant risk factors for PRES.
Small-fiber neuropathies are very painful, affect unmyelinated C-fiber nerve, and, although common, are underdiagnosed in SLE. Nerve conduction studies are normal, and small-fiber deficits appear on physical examination. A punch skin biopsy showing a decreased density of small-fiber nerves in the epidermal layer is diagnostic. There are two patterns of small-fiber neuropathies in SLE: length-dependent, affecting distal-most axons, and non-length-dependent, affecting proximal dorsal root ganglia.
There are two types of myelitis in SLE: gray-matter myelitis and white-matter myelitis. The distinguishing characteristics are summarized in Table 1.
Summary of Distinguishing Differences Between Gray-Matter and White-Matter Myelitis
Gray-matter myelitis is caused by catastrophic venous hypertension in which blood flow to the spinal cord is impaired and necrosis occurs. Dr. Birnbaum pointed out that 9 of 11 patients they identified had sought medical attention for the inability to void, and were ambulatory at the time. Many were sent home with a catheter. He emphasized that unexplained inability to void in patients with highly active SLE should be taken as a sign of impending spinal cord herniation; patients should be treated immediately with pulsed intravenous steroids to avoid irreversible paraplegia.
MANAGING DERMATOLOGIC MANIFESTATIONS OF SLE
M. Kari Connolly, MD, University of California, San Francisco, California, USA, described severe cutaneous manifestations in patients with SLE, pointing out that the presentations of skin complications may be atypical or suggest other diagnoses. The differential diagnosis should include infection, drug rash, erythema multiforme, small-vessel vasculitis, bullous LE, and acute flare of SLE. Skin biopsy cannot differentiate SLE subtypes, but can differentiate SLE from other diagnoses, distinguish inflammation from scarring, and detect the presence of microthrombi or leukocytic vasculitis.
When SLE is refractory to standard therapies like antimalarials, thalidomide may be effective [Cuadrado MJ et al. Am J Med 2005]. It requires enrollment in a safety program due to its teratogenicity; it can also cause neuropathy [Bastuji-Garin S et al. J Invest Dermatol 2002]. Maintenance therapy is usually needed. Lenalidomide, a newer thalidomide analogue, is also effective; neutropenia is a significant toxicity and necessitates regular blood counts [Cortés-Hernandez J et al. Arthritis Res Ther 2012]. Topical steroids, tacrolimus, pimicolimus, and retinoids, may also be effective.
Bullous LE is rare, nonscarring, and involves neutrophils rather than leukocytes. The immunomodulator dapsone is effective, but may require combination therapy with prednisone, mycophenolate, azathioprine, or rituximab [Hall RP et al. Ann Intern Med 1982; Ludgate MW Greig DE. Australas J Dermatol 2008]. Dapsone causes hemolytic anemia in 20% of patients and requires testing for glucose-6-dehydrogenase. LE panniculitis is also rare, and is associated with characteristic saucer-shaped deformities. The differential diagnosis includes subcutaneous T cell lymphoma. The associated deformities do not respond well to cosmetic surgery, lasers, or fillers, or to kenalog injections. Other SLE therapies may be effective.
Dr. Connolly said that dermatologists can help other clinicians by determining what is scar tissue and what is active disease (eg, when areas of hair loss are no longer treatable). Dermatologists are good at performing biopsies and experienced in the use of agents with which rheumatologists may be less familiar.
Some complications of SLE can be managed, including thrombocytopenia. Gray-matter myelitis that may present as an inability to void should be treated immediately to prevent permanent paraplegia. Other complications of SLE, such as atherosclerosis, a major cause of death, does not respond to statin therapy, so other therapies are needed, as they are for other symptoms that are important to patients, including fatigue and cognitive impairment.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.