

Summary
Triple disease-modifying antirheumatic drug (DMARD) therapy is superior to methotrexate monotherapy on measures of disease activity as initial treatment for rheumatoid arthritis (RA). The design and results of the multicenter stratified single-blind Treatment in the Rotterdam Early Arthritis Cohort trial [tREACH] comparing treatment strategies, including different glucocorticoid bridging therapies, in adults with early RA are discussed in this article
- Rheumatology Clinical Trials
- Rheumatoid Arthritis
- Rheumatology Clinical Trials
- Rheumatology
- Rheumatoid Arthritis
Triple disease-modifying antirheumatic drug (DMARD) therapy is superior to methotrexate (MTX) monotherapy on measures of disease activity as initial treatment for rheumatoid arthritis (RA).
The design and results of the multicenter stratified single-blind Treatment in the Rotterdam Early Arthritis Cohort trial [tREACH] comparing treatment strategies, including different glucocorticoid bridging therapies, in adults with early RA were discussed by Pascal H.P. de Jong, MD, Erasmus University Medical Center, Rotterdam, The Netherlands.
In 2010, the European League Against Rheumatology recommended MTX monotherapy rather than a combination of DMARDs as an initial treatment strategy for RA [Smolen Js et al. Ann Rheum Dis 2010], although several clinical trials concluded that initial combination therapy had superior clinical efficacy over monotherapy. The principal motive for disregarding combination therapy were the fact that trials were biased by glucocorticoids and there were safety concerns. There is also not much data on the optimal glucocorticoid dosage and/or tapering scheme, noted Prof. de Jong.
The tREACH trial compared three treat-to-target strategies in 281 adults who had a high probability of progressing to persistent arthritis based on the Visser prediction model. Interestingly, the Visser algorithm and 2010 criteria for RA have similar discriminative abilities to identify patients at risk of persistent arthritis. Patients were randomized to one of three strategies:
-
▪ Arm A (n=91): Triple DMARD therapy (MTX, sulfasalazine, and hydroxychloroquine) with one-time administration of intramuscular glucocorticoids
-
▪ Arm B (n=93): Triple DMARD therapy with an oral glucocorticoid tapering scheme, starting at 15 mg/day
-
▪ Arm C (n=97): MTX with oral glucocorticoids as in Arm B
Patients were followed every 3 months, with treatment decisions designed to maintain a disease activity score (DAS) <2.4. In the event of treatment failure, defined as DAS ≥2.4, the medication regimen was intensified to include biologic agents. In cases of sustained remission, defined as DAS <1.6 at two consecutive visits, medication was tapered. The mean symptom duration of participants was 166 days and the mean DAS at baseline ranged from 3.28 to 3.40. Women comprised 68% of the study populationw.
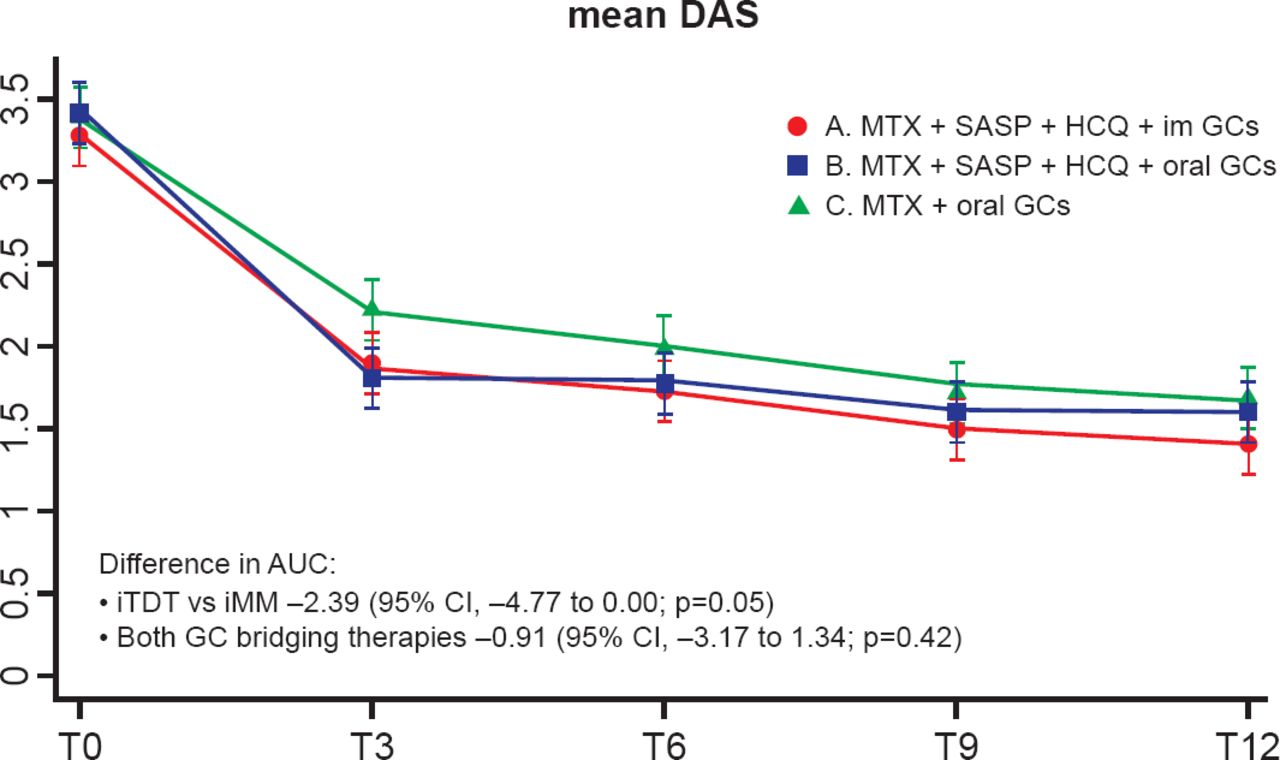
The difference in disease activity over time, as measured by area under the curve (AUC) for mean DAS score, was −2.39 in favor of the triple DMARD strategy (p=0.05; Figure 1). The largest difference in disease activity between groups occurred at 3 months indicating that treatment goals were achieved faster with triple DMARD therapy. The difference after 3 months diminished because of the treat-to-target approach in all groups, necessitating intensification of treatment in Arm C, explained Prof. de Jong. There was no difference on this outcome between the two glucocorticoid bridging strategies. Functional ability, as measured by the AUC for mean scores on the Health Assessment Questionnaire, was again superior with triple DMARD therapy versus MTX monotherapy (difference: 1.67; p=0.05), again with no difference on this measure between the two glucocorticoid strategies.

Change in Disease Activity
AUC=area under the curve; DAS=disease activity score; GC=glucocorticoid;
HCQ=hydroxychloroquine; im=intramuscular; iMM=initial MTX monotherapy;
iTDT=initial triple disease-modifying antirheumatic drug therapy; MTX=methotrexate;
SASP=sulfasalazine.
Reproduced with permission from PHP de Jong, MD.
Radiographic progression after 1 year occurred in 19%, 23%, and 21% of patients in Arms A, B, and C, respectively.
At 3 months, there were fewer treatment failures in the triple DMARD therapy groups, resulting in the prescription of ∼40% fewer biological medications, and this difference remained over time.
At 12 months, use of biological medications was 29% in Arm A, 26% in Arm B, and 43% in Arm C. There were no differences between groups in serious adverse events and no difference in dosage adjustments per drug due to adverse events.
Prof. de Jong concluded that treatment goals are attained faster and are maintained with the need for fewer biologic agents in RA patients started on triple DMARD therapy compared with MTX monotherapy.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.