

Summary
This article discusses the role of the autonomic nervous system in the development of refractory hypertension and its relation to renal denervation, as well as a scientific update on renal denervation, a review of products in various stages of commercial development, and future prospects for renal denervation therapy.
- Interventional Techniques & Devices Renal Disease
- Hypertension & Kidney Disease
- Hypertensive Disease
- Interventional Radiology
Michael Böhm, MD, Universitätsklinikum des Saarlandes, Saarbrücken, Germany, discussed the role of the autonomic nervous system in the development of refractory hypertension and its relation to renal denervation.
Engagement of the “fight or flight” response in the sympathetic nervous system (SNS) has wide-ranging effects that include accelerated heartbeat, conversion of glycogen to glucose, and secretion of adrenaline and noradrenaline. Sustained heightened central nervous system (CNS) sympathetic activity is likely to play an integral role in the development of hypertension and its complications [Smith PA et al. Am J Hypertens 2004].
In an 18-year follow-up study, Flaa at al. [Hypertension 2008] found that sympathoadrenal stress reactivity is a predictor of future blood pressure (BP) and probably plays a key role in the pathogenesis of essential hypertension.
Similarly, a prospective study assessing the relationship between sympathetic activity and the development of hypertension demonstrated that a higher resting noradrenaline concentration was associated with the development of hypertension during a 7-year follow-up [Böhm RO et al. J Hypertens 1987].
Prof. Böhm's key messages were that the “fight and run” SNS is elevated in hypertension; afferent renal nerves are mechanisms of SNS activation; and the SNS is overactive in renal and heart failure, sleep apnea, and metabolic syndrome. He believes renal nerve ablation is a feasible way to reduce SNS overactivity.
Critical Appraisal of the Clinical Data
Deepak L. Bhatt, MD, MPH, Harvard Medical School, Boston, Massachusetts, USA, gave a scientific update on renal denervation. The most commonly accepted definition of resistant hypertension is uncontrolled BP despite the use of drugs from 3 or more antihypertensive classes (1 of which is a diuretic) at maximally tolerated doses [Bhatt DL, Bakris GL. Cleve Clin J Med 2012]. About 1 in 50 patients with a new diagnosis of hypertension will develop resistant hypertension [Daugherty SL et al. Circulation 2012].
Sympathetic drive from the CNS acts on the kidney to decrease renal blood flow, increase sodium retention, and stimulate renin release. Afferent renal nerves make the kidney a source of central sympathetic activity, sending signals to the CNS [Schlaich MP et al. Hypertension 2009; Figure 1].

Renal Injury can Induce Activation of Sensory Afferent Signals.
Reproduced from Schlaich MP et al. Renal Denervetion as a Therapeutic Approach for Hypertension: Novel Implication for an Old Concept. Hypertension 2009; 54 1195–1201, with permission from Elsevier.
Dr. Bhatt discussed critical issues remaining about renal denervation, including estimated effect size, durability, predictors of response, and the limitations of existing data. Based on the latest data, renal denervation seems promising although longer follow-up data are needed. Competitive devices are being investigated with positive early data. The Renal Denervation in Patients with Uncontrolled Hypertension [SYMPLICITY HTN-3; NCT01418261] trial is currently enrolling and will be the pivotal study for the US Food and Drug Administration on which to base its approval, and will address many of the limitations of prior studies.
Catheter-Based Technology Alternatives for Renal Denervation
Horst Sievert, MD, CardioVascular Center Frankfurt, Frankfurt, Germany, reviewed products in various stages of commercial development.
A renal denervation device that uses multi-electrode radio frequency (RF) with simultaneous firing and 60-second ablation time per artery is currently being studied. The Multi-electrode Radiofrequency Renal Denervation System Feasibility Study [NCT01699529] is a prospective, single-arm, nonrandomized, open-label feasibility study. It intends to evaluate the safety and efficacy of multi-electrode RF renal denervation in patients with uncontrolled hypertension. The primary outcome is acute safety as measured by procedural complications within 1 month. The secondary outcome is change in office systolic BP from baseline to 6 months. A first-in-man trial with 9 patients has been completed in Australia.
Another renal denervation system uses a balloon catheter with a spiral electrode. The catheter is a 0.014 inch compatible, 20 mm long balloon that comes in 5, 6, and 7 mm diameters. Cooling is achieved by irrigation holes placed alongside the spiral electrodes. The cooling protects the nontreated region of the artery, enhances control and consistency of the treatment effect, and prevents the electrode from adhering to tissue. Ablation takes 2 minutes per artery.
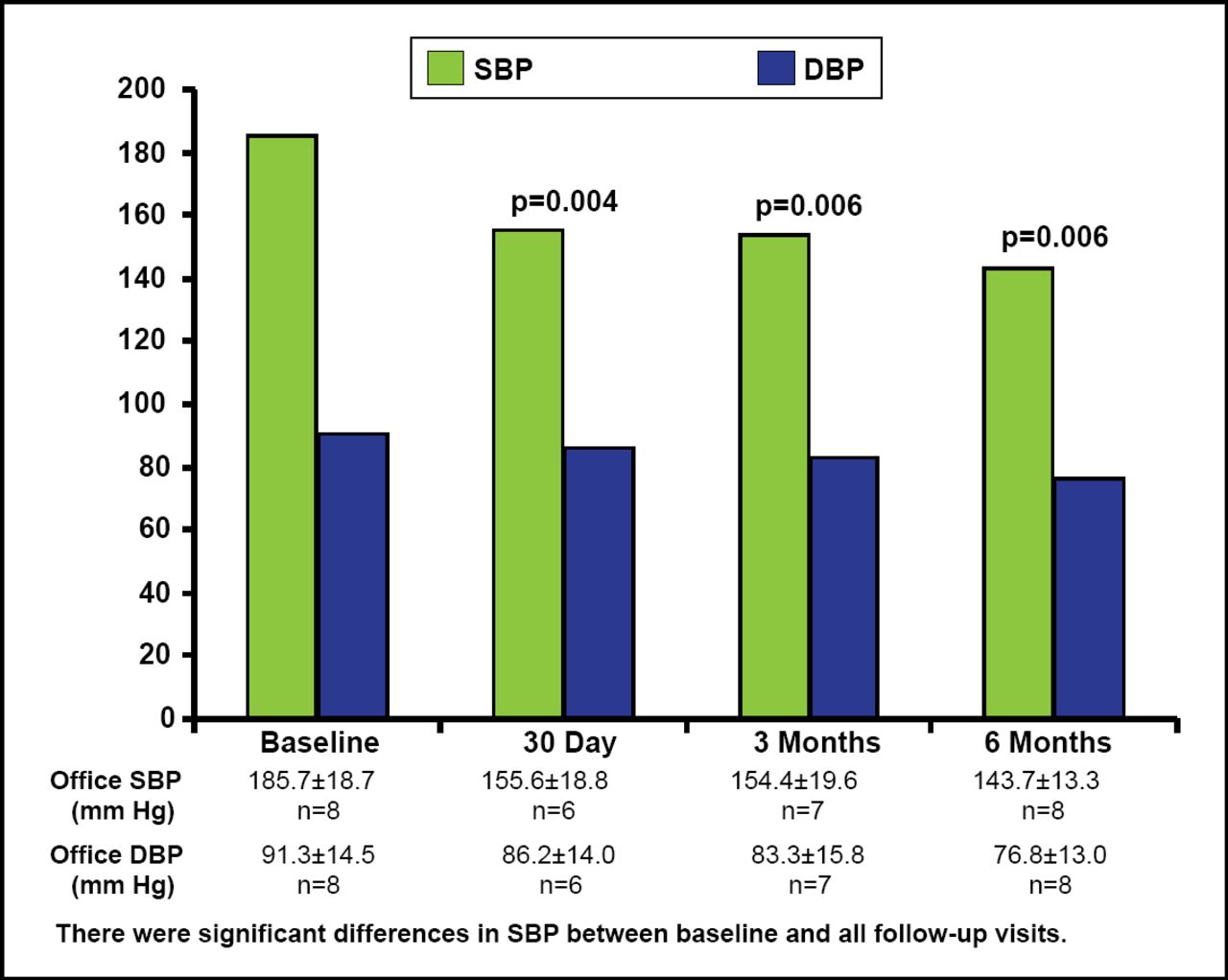
In the first patient treated with this device, the balloon was inflated to 1 atmosphere (atm) for 2 minute ablation on each side of the artery. In a pilot trial (n=8) there were significant reductions in systolic BP between baseline and all follow-up visits (Figure 1). Recruitment for the phase 2, multicenter Rapid Renal Sympathetic Denervation for Resistant Hypertension trial [RAPID; NCT01520506] is currently under way. The purpose of the study is to deliver low-level RF energy through the wall of the renal artery to denervate the human kidney. The primary outcome measures of the open-label, single-group assignment safety/efficacy study are acute procedural safety in 1 week and acute procedural safety, defined as the overall rate of serious adverse events (SAEs) and adverse device effects at discharge (eg, SAEs related to groin and vascular access complications, and SAEs related to renal artery injury). Estimated enrollment is 40 patients.
A balloon catheter with bipolar RF electrodes is designed to simultaneously deliver energy to all electrodes at low temperature (68°C) and low pressure (<3 atm). Designed for 3- to 7-mm renal arteries, treatment time is 30 seconds at 1 watt maximum. A pilot study cohort of 13 patients treated at 6 centers showed significant declines in BP, and patients are currently being recruited for the Treatment Resistant Hypertension Using a Radiofrequency Percutaneous Transluminal Angioplasty Catheter trial [REDUCE-HTN; NCT01541865]. The objective of the single group assignment, open-label, multicenter post-market approval clinical safety/efficacy study is to assess the performance of this system for the treatment of uncontrolled hypertension using an innovative percutaneous RF balloon catheter renal denervation device. The primary outcome measure is a change in systolic and diastolic BP at 6 months compared with baseline. The secondary outcome measure is the absence of flow limiting stenosis in the renal artery at 6 months compared with baseline. Estimated enrollment is 120 patients.
Degradable botulinum toxin type B nanoparticles (∼100 nm) are being tested in animal models, using a paramagnetic core with polymeric coating. Particles are injected into the renal artery and pulled into the artery wall by a magnetic field. The 2 possible mechanisms are heat-generated by the magnetic field or the botulinum toxin type B released by the particles. Animal trials will start at the end of 2012.
Other technologies in development use radiation or ultrasound techniques, including sound intervention.
Beyond Hypertension: Future Prospects for Renal Denervation Therapy
While discussing the future prospects for renal denervation therapy, Paul A. Sobotka, MD, Ohio State University, Columbus, Ohio, USA, identified 3 main areas: prevention of hypertension and insulin resistance; symptom reduction of tachyarrhythmia, atrial fibrillation, and venous thromboembolism; and mortality reduction from chronic kidney and other cardiorenal syndromes.
He pointed out that important technical questions remain unanswered, including whether reduction of either renal sympathetic efferent and/or afferent signals is desirable and what the optimal dose of efferent and afferent denervation across various patient populations and clinical endpoints may be (eg, complete denervation may not be desirable, or changes in the mode of denervation may alter the mix of afferent and efferent denervation).
The afferent-efferent debate has implications— whether benefits of renal denervation are embedded in reduction of renal sympathetic efferent signaling or in the reduction of renal afferent signaling to the CNS. Dr. Sobotka envisions an endovascular procedure to protect a single organ from the ravages of excessive sympathetic stimulation and/or reduce central sympathetic drive by the selective reduction of a single organ's contribution.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.