

Summary
Results from the Placement of Aortic Transcatheter Valve Trial [PARTNER B; NCT00530894] continue to support the role of transcatheter aortic valve replacement as the standard of care for symptomatic patients with aortic stenosis who are not surgical candidates, as presented 3-year follow-up findings from the PARTNER B trial.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Valvular Disease
Results from the Placement of Aortic Transcatheter Valve Trial [PARTNER B; NCT00530894] continue to support the role of transcatheter aortic valve replacement (TAVR) as the standard of care for symptomatic patients with aortic stenosis who are not surgical candidates, said E. Murat Tuzcu, MD, Cleveland Clinic, Cleveland, Ohio, USA. Dr. Tuzcu presented 3-year follow-up findings from the PARTNER B trial.
The objectives of the trial were to evaluate the clinical outcomes of TAVR compared with standard therapy at 3 years in patients with inoperable aortic stenosis (iAS), to assess valve hemodynamics and durability using echocardiography, and to perform subgroup analyses to better define the impact of comorbidities on outcomes.
A total of 358 patients with iAS were randomized (1:1) to receive a transcather heart valve or standard medical therapy. The inclusion criteria were severe calcific aortic stenosis, defined as an echo-derived valve area of <0.8 cm2 (effective orifice area index <0.5 cm2/m2), and mean gradient >40 mm Hg or jet velocity >4.0 m/s; NYHA Class ≥II; and inoperable, defined as risk of death or serious irreversible morbidity with surgical replacement >50% as assessed by a cardiologist and 2 surgeons.
Key endpoints for the 3-year analysis were all-cause and cardiac mortality; rehospitalization; adverse outcomes, including stroke, bleeding, renal failure, or myocardial infarction; NYHA functional class; days alive and out of hospital; echo-derived valve areas, transvalvular gradients, and post-TAVR aortic regurgitation; and mortality outcomes stratified by the Society of Thoracic Surgeons mortality risk score.
Baseline characteristics were similar between the 2 groups. The mean age was 83 years, and nearly half (46%) of the subjects were men. Patients in the standard-care group had significantly higher rates of chronic obstructive pulmonary disease compared with the TAVR group (52.5% vs 41.3%, respectively; p=0.04) and atrial fibrillation (48.8% vs 32.9%; p=0.04). The prevalence of porcelain aorta was 19.0% in the TAVR group versus 11.2% in the standard-care group (p=0.05).
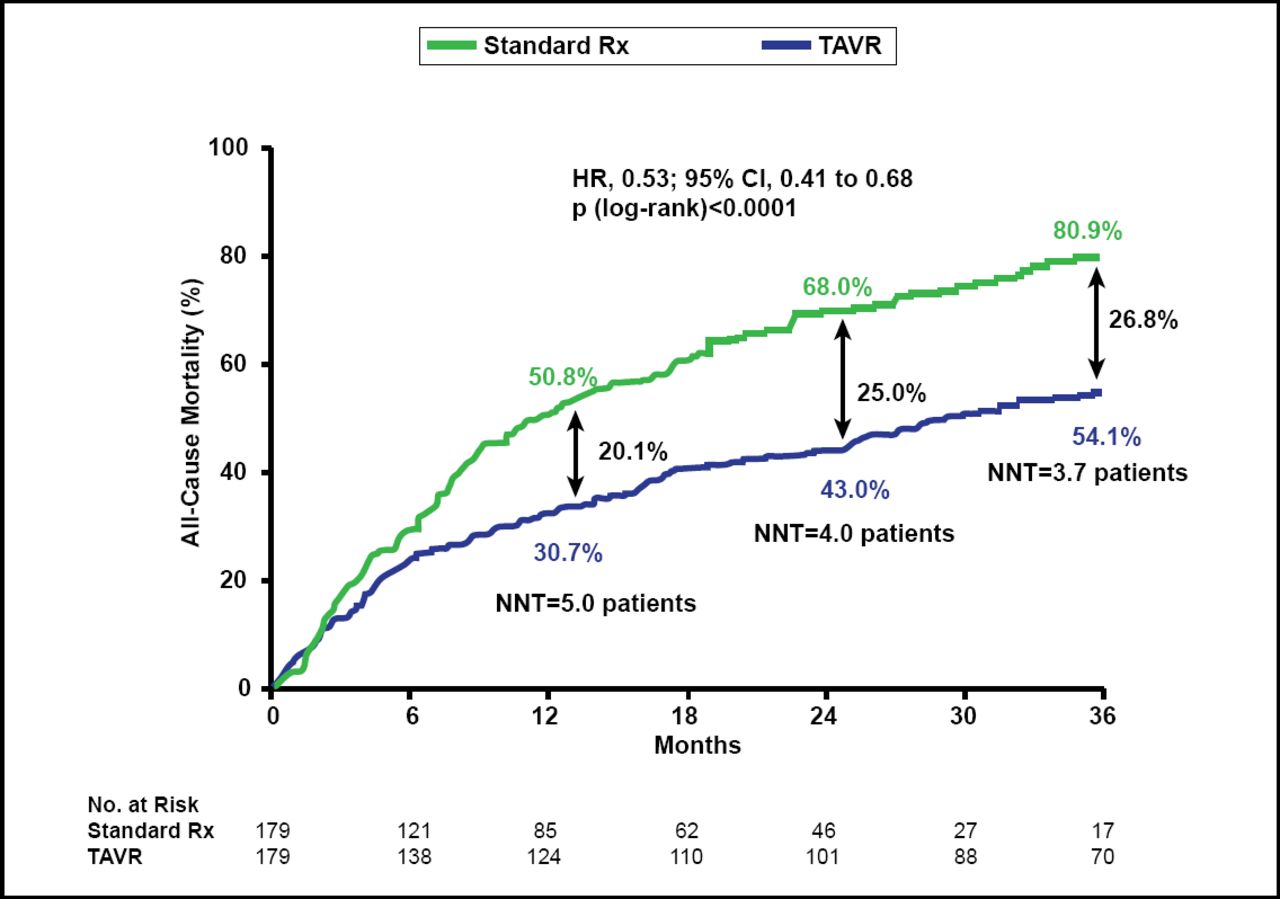
The Kaplan-Meier estimated rates of all-cause mortality at 3 years were 80.9% in the standard-care arm versus 54.1% in the TAVR arm, an absolute reduction of 26.8% (HR, 0.53; 95% CI, 0.41 to 0.68; log-rank p<0.0001). The number needed to treat (NNT) was 3.7 patients (Figure 1). Rates for cardiovascular mortality were similarly reduced from 74.5% to 41.4%, a 33.1% reduction with an NNT of 3.0 patients. Serial landmark analyses performed at baseline, 12 months, and 24 months demonstrate a consistent, significant reduction in all-cause mortality for TAVR as compared with standard care.

Figure 1. All-Cause Mortality (ITT): Crossover Patients Censored at Crossover.
ITT=intention-to-treat; TAVR= transcatheter aortic valve replacement.
Reproduced with permission from EM Tuzcu, MD.
Based on the data, Dr. Tuzcu concluded that the benefits of TAVR as measured by all-cause mortality, cardiovascular mortality, repeat hospitalization, and functional status were sustained through 3 years of follow-up. Durability of the implanted valves was also demonstrated with no increase in transvalvular gradient or attrition of valve area. Detailed analysis of all randomized inoperable patients showed consistent results for all outcomes. He also noted that survival benefit of TAVR is dependent on the presence of comorbid illness and, without TAVR, mortality is similar irrespective of comorbid illness.
Three-year outcomes continue to support the role of TAVR as the standard of care for symptomatic patients with aortic stenosis who are not surgical candidates. “These data underscore the importance of patient selection before TAVR and the need for aggressive management of illnesses after TAVR,” said Dr. Tuzcu.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.