

Summary
An analysis from the Assessment of Dual Antiplatelet Therapy with Drug-Eluting Stents [ADAPT-DES; NCT00638794] trial showed that hyporesponsiveness to clopidogrel was not independently predictive of mortality at 1-year after percutaneous coronary intervention with a drug-eluting stent. Although hyporesponsiveness to clopidogrel was associated with increased risk of stent thrombosis and myocardial infarction, it was also associated with a reduced risk of major bleeding, which has been strongly related to mortality.
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Thrombotic Disorders
An analysis from the Assessment of Dual Antiplatelet Therapy with Drug-Eluting Stents [ADAPT-DES; NCT00638794] trial showed that hyporesponsiveness to clopidogrel was not independently predictive of mortality at 1-year after percutaneous coronary intervention (PCI) with a drug-eluting stent (DES). Although hyporesponsiveness to clopidogrel was associated with increased risk of stent thrombosis and myocardial infarction (MI), it was also associated with a reduced risk of major bleeding, which has been strongly related to mortality, explained Gregg W. Stone, MD, Columbia University Medical Center, NewYork-Presbyterian Hospital, New York, New York, USA.
The trial enrolled 8583 patients at 11 sites in the United States and Germany between January 2008 and September 2010. All patients had PCI with implantation of ≥1 (noninvestigational) DES. Dr. Stone said the patients in the study represented a “real-world population,” with about one-third having diabetes, one-quarter having a previous MI, and >50% having undergone a previous revascularization procedure.
The number of platelet reactivity units (PRU) and aspirin reactivity units (ARU) were assessed with the VerifyNow P2Y12 and Aspirin assays, respectively. Approximately 43% of patients were found to be hyporesponders to clopidogrel, defined as PRU >208. Hyporesponsiveness to aspirin, defined as a score of >550 ARU, was found in 5.6% of patients.
The first results of ADAPT-DES were presented last year when Dr. Stone reported that hyporesponsiveness to clopidogrel was significantly related to stent thrombosis within 30 days after PCI. The current analysis was designed to evaluate the impact of clopidogrel hyporesponsiveness on patient outcomes after 1 year of follow-up.
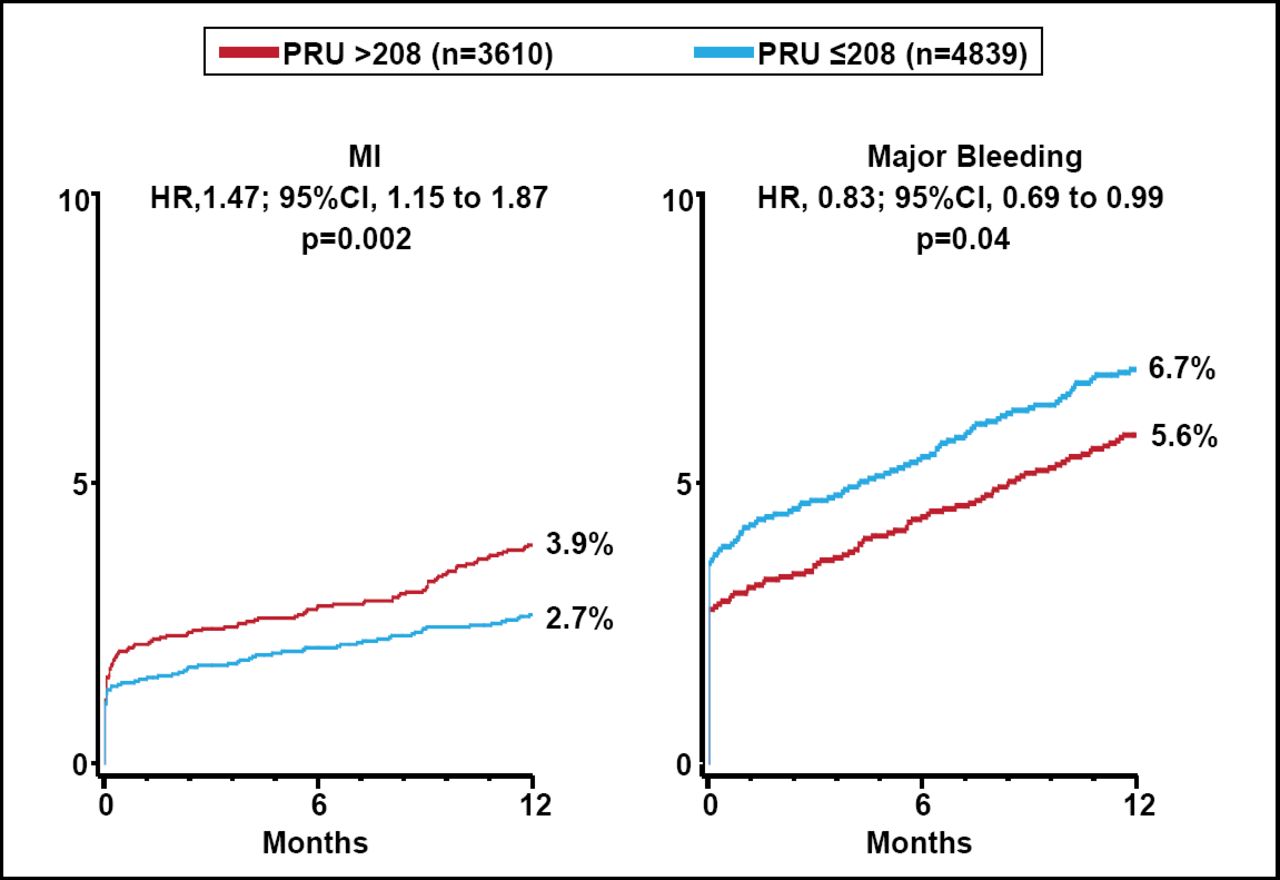
At 1 year, 74 stent thrombosis events had occurred in 70 patients (0.84%), MI had occurred in 224 patients (2.6%), major bleeding had occurred in 531 patients (6.2%), and 161 patients had died (1.9%). The rate of stent thrombosis was significantly higher for patients who were hyporesponsive to clopidogrel than for those with a PRU ≤208 (1.3% vs 0.5%; HR, 2.54; 95% CI, 1.55 to 4.16; p=0.0001). The rate of MI was also significantly higher for the group with hyporesponsiveness (3.9% vs 2.7%; HR, 1.47; 95% CI, 1.15 to 1.87; p=0.002).
In contrast, patients with hyporesponsiveness to clopidogrel had significantly lower rates of major bleeding (5.6% vs 6.7%; HR, 0.83; 95% CI, 0.69 to 0.99; p=0.04; Figure 1)

ADAPT-DES: MI and Major Bleeding According to Post-PCI PRU.
MI=myocardial infarction; PCI=percutaneous coronary intervention; PRU=platelet reactivity units; Reproduced with permission from GW Stone, MD.
Hyporesponsiveness to aspirin predicted a slightly lower risk of bleeding but did not predict a difference in stent thrombosis, MI, or mortality. Dr. Stone noted that this finding raises the question of whether aspirin is of benefit for patients treated with a DES.
Univariable analysis showed that hyporesponsiveness to clopidogrel was significantly associated with mortality, with a rate of 2.4% for patients with a PRU >208 compared with 1.5% for those patients with a PRU <208 (HR, 1.62; 95% CI, 1.18 to 2.22; p=0.002). However, he added that a number of factors associated with hyporesponsiveness are also associated with mortality (eg, age and diabetes). To address this issue, he and his coinvestigators performed a propensity adjustment for hyporesponsiveness to clopidogrel. A multivariable propensity score adjusted risk model demonstrated no independent association between hyporesponsiveness to clopidogrel and mortality (adjusted HR, 1.20; 95% CI, 0.85 to 1.70; p=0.30). Stent thrombosis, MI, and major bleeding remained significantly associated with hyporesponsiveness to clopidogrel in this analysis (p=0.001, p=0.01, and p=0.002, respectively).
Dr. Stone said that many more deaths were associated with major bleeding than with stent thrombosis and MI combined. He added that a complete effect in reversing hyporesponsiveness to clopidogrel would cause 4 bleeding events for every stent thrombosis prevented. He and his coinvestigators concluded that the findings suggest that the use of potent antiplatelet agents to overcome hyporesponsiveness to clopidogrel is unlikely to improve survival unless the beneficial effects of reducing stent thrombosis and MI can be uncoupled from the likely increase in bleeding.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.