

Summary
The clinical value of achieving no evidence of disease (NED) in patients with advanced colorectal cancer (depends on the balance between the duration of the NED state and the toxicity of the treatments to achieve it, particularly with multimodal interventions. This article discusses the rationale for pursuing the NED state and factors to consider in the decision to pursue this goal.
- Gastrointestinal Cancers
The clinical value of achieving no evidence of disease (NED) in patients with advanced colorectal cancer (CRC) depends on the balance between the duration of the NED state and the toxicity of the treatments to achieve it, particularly with multimodal interventions. Alberto Sobrero, MD, Hospital San Martino, Genova, Italy, discussed the rationale for pursuing the NED state and factors to consider in the decision to pursue this goal.
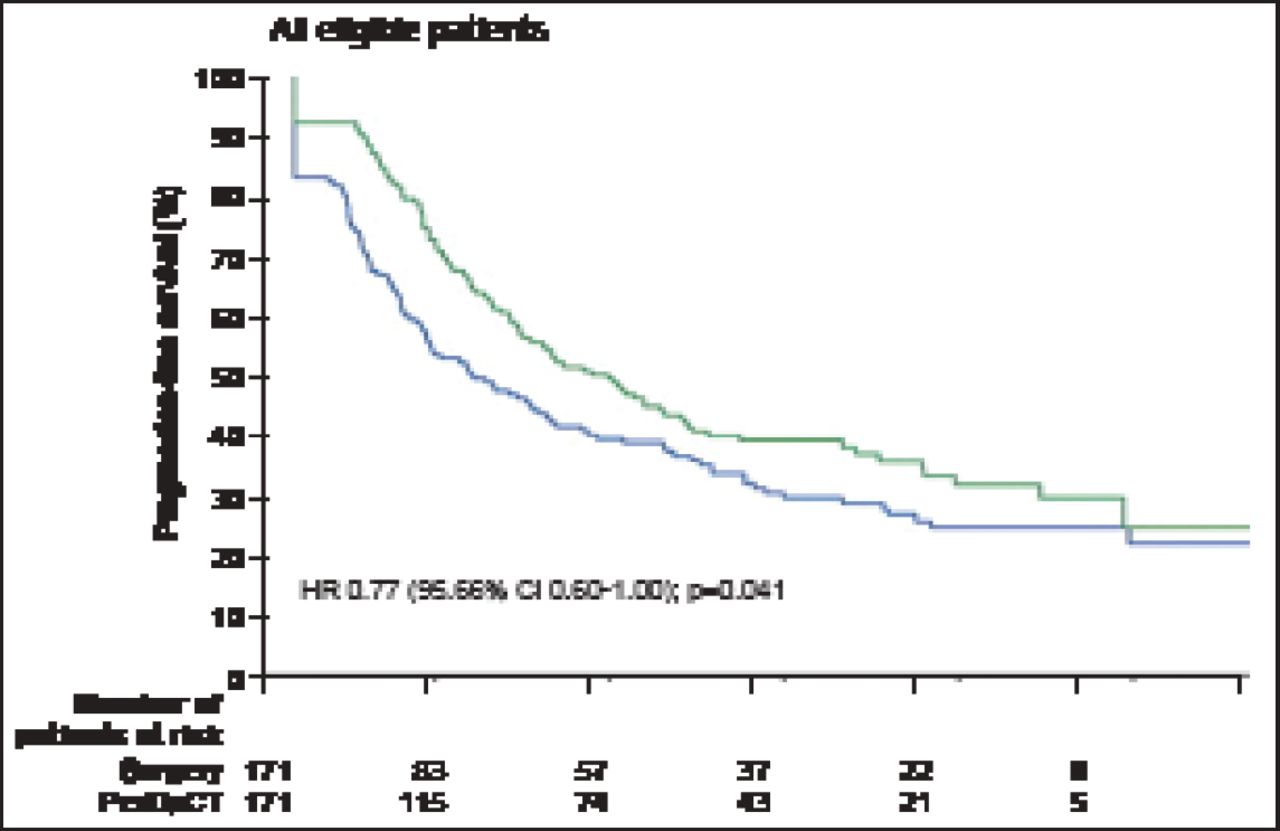
The chance of achieving NED is marginal with systemic therapy alone but substantial with local approaches. However, local approaches can be toxic and the addition of adjuvant chemotherapy after local treatment is not as effective as it should be. Results of a pooled analysis from two trials of 278 patients with advanced CRC showed that patients treated with surgery and adjuvant 5-fluorouracil (5-FU) chemotherapy had a 7% higher progression-free survival (PFS) rate than those treated with surgery alone (p=0.058) [Mitry E et al. J Clin Oncol 2008]. Nordlinger et al. [Lancet 2008] reported an 8.1% improvement in PFS at 3 years in patients with advanced CRC treated with surgery and perioperative chemotherapy versus surgery alone (HR, 0.77; 95% CI, 0.60 to 1.00; p=0.041; Figure 1). Another study found no significant difference in disease-free survival between patients treated with 5-FU/folinic acid (LV5FU) alone versus LV5FU plus irinotecan (HR, 0.89; 95% CI, 0.66 to 1.19) [Ychou M et al. ASCO 2008. Abstract LBA4013].

PFS at 3 Years: All Eligible Patients.
Reprinted from Nordlinger B et al. Perioperative Chemotherapy with FOLFOX4 and Surgery Versus Surgery Alone for Resectable Liver Metastases from Colorectal Cancer (EORTC Intergroup Trial 40983): A Randomised Controlled Trial. The Lancet;371(9617):1007–16. Copyright 2008, with permission from Elsevier.
Achieving NED for at least 12 months gives patients hope for a cure, and is considered beneficial and relevant, whereas the value of achieving NED for 6 months is questionable and for <6 months, can be harmful. In a highly selected population of patients treated with surgery for liver metastases, 5- and 10-year survival rates were 40% and 20% for overall survival (OS), and 20% and 10% for relapse-free survival (RFS). Among unselected patients, the actual cure rate ranged from 1% to 4%.
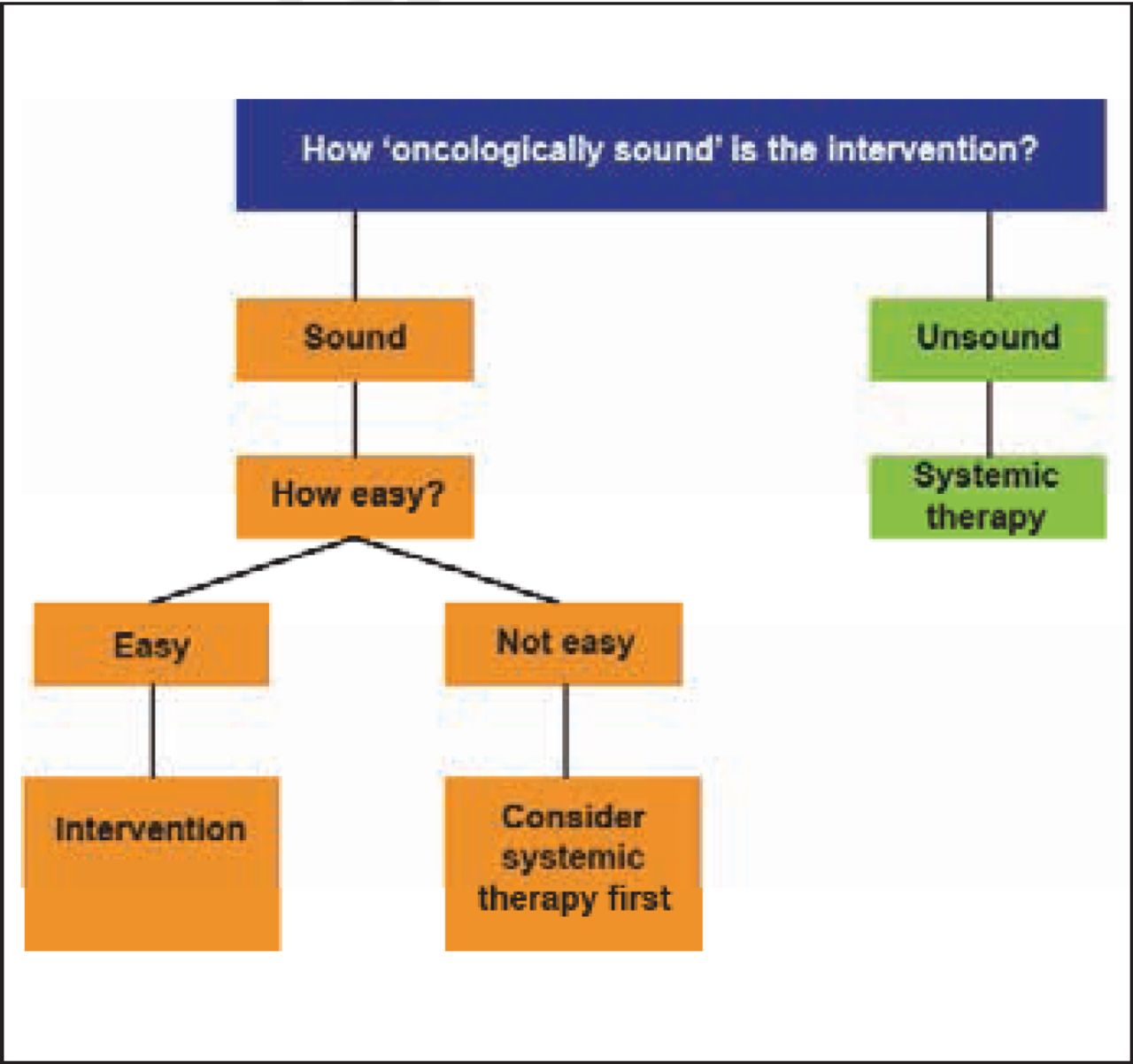
Prof. Sobrero cautioned against using overly aggressive local treatment approaches because of the high rate of failure to achieve a NED state, the typically very short RFS, possible acceleration of the clinical course, treatment complications, and high mortality. Verwaal et al. [Ann Surg Oncol 2005] concluded that the key issue in selecting patients for cytoreduction and adjuvant therapy is selecting patients in whom it is feasible to reach complete cytoreduction. Laparotomy to diagnose peritoneal carcinomatosis provides the best information for selecting such candidates. According to Prof. Sobrero, this is an example of a simplified approach that can be generalized and used to determine the chance of achieving relevant NED, by evaluating the “soundness” of an intervention and the ease of performing the intervention (Figure 2).

A Simplified Approach to Determine Chance of Achieving Relevant No Evidence of Disease.
Reproduced with permission from A Sobrero, MD.
High originality and relevance coupled with low intrinsic and external validity of the results are the classic features and limits of most trials in this patient population. The main hurdles facing clinical trials in this field are poor feasibility and methodology. Trials must be designed to minimize bias (systematic error) and variability (random error). Bias can be minimized by randomization, treatment masking, eligibility criteria, and intention-to-treat analysis. Variability can be minimized by randomization, the number of patients, target delta, and patient stratification. However, these methods of minimizing bias and variability can be difficult to implement in this field.
Prof. Sobrero concluded that achieving the NED condition in patients with advanced CRC is very relevant. Physicians should not deceive themselves and patients but should, instead, aim for plausible results. The goal includes identifying appropriate patients for this approach, recognizing but not being paralyzed by the limitations of clinical trials in this field, and taking into consideration the toxicities associated with local therapy.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.