

Summary
Final results of the Induction Therapy with Methotrexate and Prednisone in Rheumatoid or Very Early Arthritis Disease [IMPROVED] study showed that patients with rheumatoid arthritis and undifferentiated arthritis achieved similarly greater rates of remission after early initial treatment with combination therapy (methotrexate and prednisone). Patients who failed to achieve early remission benefited more when switched to a treatment strategy with adalimumab than with multiple disease modifying antirheumatic drugs, with virtually no radiographic damage progression in all patients.
- Rheumatology Clinical Trials
- Rheumatoid Arthritis
Final results of the Induction Therapy with Methotrexate and Prednisone in Rheumatoid or Very Early Arthritis Disease [IMPROVED] study, reported by Lotte Heimans, MD, Leiden University Medical Center, Leiden, The Netherlands, showed that patients with rheumatoid arthritis (RA) and undifferentiated arthritis (UA) achieved similarly greater rates of remission after early initial treatment with combination therapy (methotrexate [MTX] and prednisone). Patients who failed to achieve early remission benefited more when switched to a treatment strategy with adalimumab than with multiple disease modifying antirheumatic drugs (DMARDs), with virtually no radiographic damage progression in all patients.
The objectives of the IMPROVED trial were to assess if induction of remission and drug-free remission is possible with initial combination therapy in early RA and UA, to determine which strategy results in more remission if the initial combination fails, and to compare results in RA and UA patients. The study included adult patients with RA (2010 criteria; n=479) of <2 years duration or rheumatologist-determined UA (n=122). The goal was remission (Disease Activity Score [DAS] <1.6).
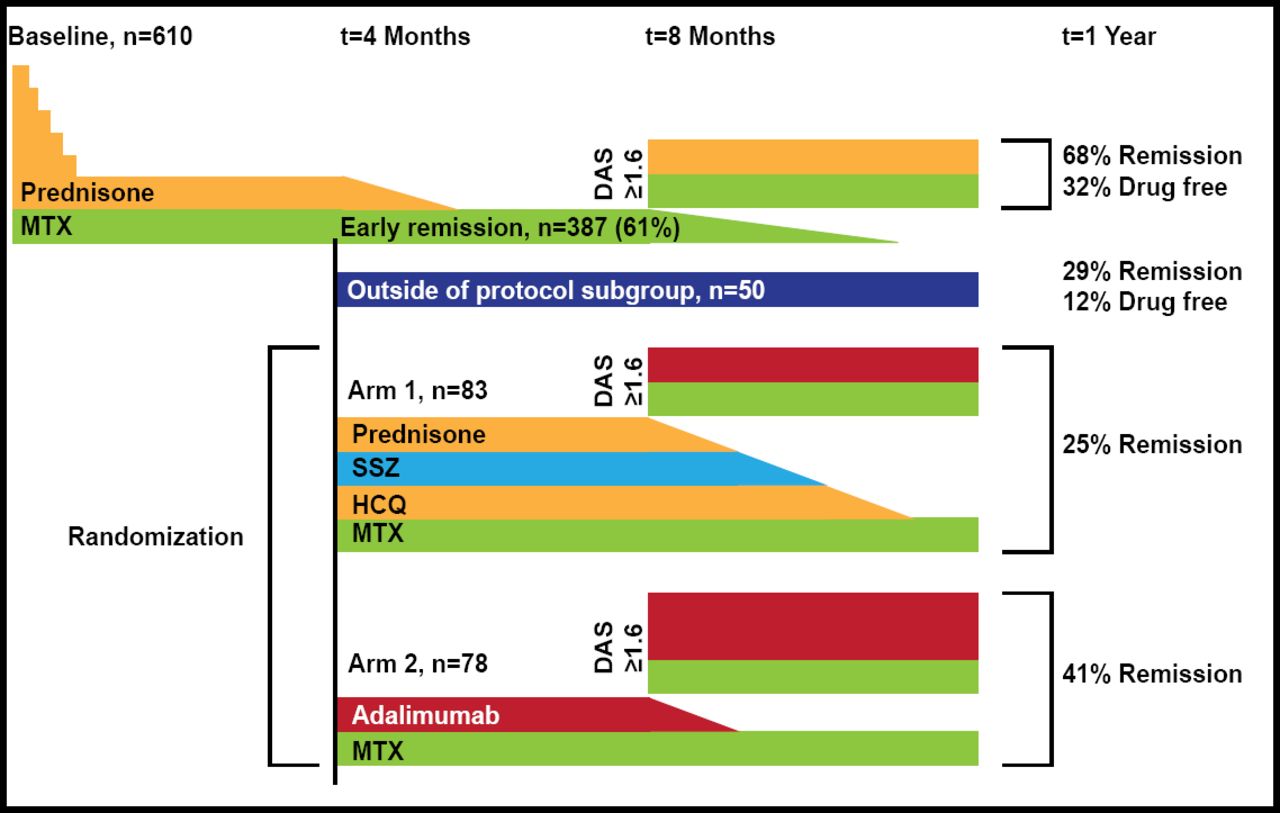
All patients were initially treated with MTX (25 mg QW) and prednisone (60 mg QD tapered to 7.5 mg QD over 7 weeks). Prednisone was tapered then discontinued for patients with a DAS <1.6 at 4 months. MTX was tapered for patients with a DAS <1.6 at 8 months. If remission was lost after 8 months, prednisone was restarted at 7.5 mg QD. Patients not in remission at 4 months were randomized to Arm 1 (MTX + prednisone + sulfhasalazine 2000 mg QD + hydroxychloroquine 400 mg QD [poly DMARDs + prednisone]; n=83) or Arm 2 (MTX + adalimumab [ADA] 40 mg every 2 weeks; n=78). Patients in either arm achieving remission at 8 months had their treatments tapered to MTX monotherapy. If not in remission after 8 months, patients in Arm 1 switched to ADA plus MTX and patients in Arm 2 increased ADA to 40 mg QW.
At baseline, RA patients had significantly (p≤0.02) higher DAS and Health Assessment Questionnaire scores compared with UA patients; 68% of RA patients were positive for anticitrullinated protein antibody plus (ACPA+) compared with 3% of UA patients (p<0.001). Mean age was 52 years; 70% of RA and 61% of UA patients were women; mean symptom duration was ∼17 weeks. Proportions of remission and radiographic progression measured by Sharp/van der Heijde score (SHS) after 1-year follow-up were compared between the different treatment strategies.
Early remission (4 months) was achieved by 61% of all patients (Figure 1). At 1 year, 68% of those 61% were in remission and 32% were in drug-free remission. Significantly more patients in arm 2 (MTX + ADA, 41%) achieved remission at 1 year compared with those in arm 1 (poly DMARDs + prednisone, 25%; p=0.01). There was no difference between RA (62%) and UA (65%) patients who achieved early remission (p=0.46) or 1 year remission (53% vs 58%, respectively; p=0.1). Damage progression was minimal. Only 33 patients showed a 1-point progression on SHS. Toxicity was comparable between the 2 randomized arms.

IMPROVED Study Design.
DAS=Disease Activity Score; HCQ=hydroxychloroquine; MTX=methotrexate; SSZ=sulfasalazine.
Reproduced with permission from L Heimans, MD.
In this treat-to-remission cohort, early remission more often led to remission at 1 year (radiological damage progression after 1 year and drug-free remission). Also, remission-steered therapies led to minimal radiographic damage in UA and RA patients regardless of the treatment employed.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.