

Summary
The International Diabetes Federation estimates that up to 1 adult in 10 will have diabetes by 2030 [International Diabetes Federation. IDF Diabetes Atlas. 5th ed. 2009]. To better handle this impending crisis, the latest American Diabetes Association and European Association for the Study of Diabetes guidelines present a new perspective on the management of hyperglycemia in type 2 diabetes (T2DM) [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
- Hyperglycemia/Hypoglycemia
- Nursing Diabetes & Endocrinology Guidelines
- Diabetes Mellitus
The International Diabetes Federation estimates that up to 1 adult in 10 will have diabetes by 2030 [International Diabetes Federation. IDF Diabetes Atlas. 5th ed. 2009]. To better handle this impending crisis, the latest American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD) guidelines present a new perspective on the management of hyperglycemia in type 2 diabetes (T2DM) [Inzucchi SE et al. Diabetes Care 2012; Inzucchi SE et al. Diabetologia 2012].
David R. Matthews, MD, DPhil, The Oxford Centre for Diabetes, Endocrinology and Metabolism, Oxford, United Kingdom, discussed the individualization of treatment, including the need for the new guidelines, their development, and the likely effect on the treatment of hyperglycemia.
The two organizations issued the joint statement for many reasons, including an increasing number and variety of agents, trial data that challenges the simplistic view of “the lower the better” approach to glycemic control, concerns about the safety of some medications, an algorithmic management approach that few physicians use in practice, concerns by some purchasers of health care and advisory bodies about a “one size fits all” treatment strategy, and increasing discourse about patient-centered medicine.
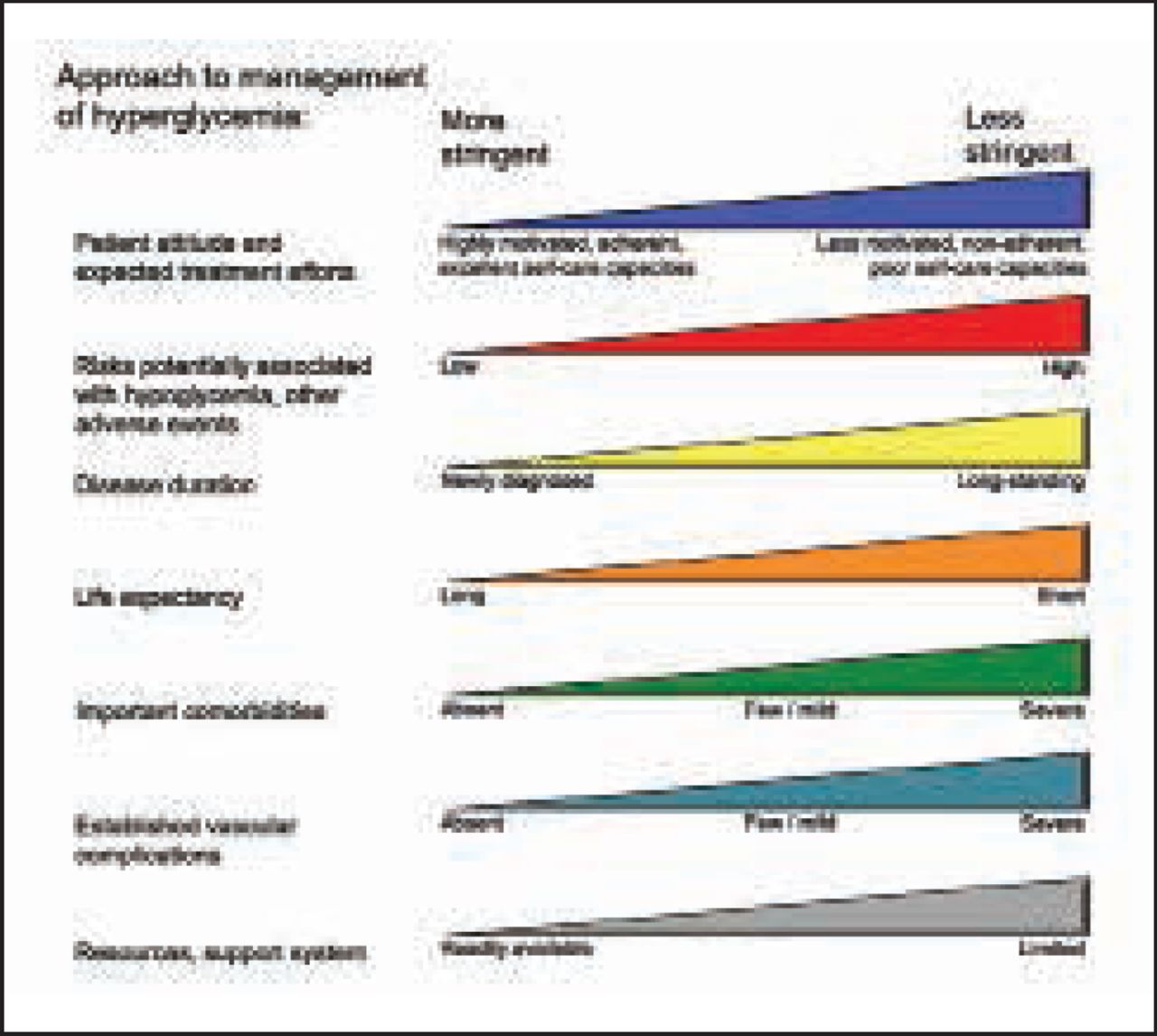
More than other previously reported guidelines, the 2012 ADA/EASD position statement clearly states that one size does not fit all [Cefalu WT. Diabetes Care 2012]. For the first time, the guidelines also stress patient preferences in the treatment process, an approach that takes into account patient attitudes, risks of therapy, disease duration, life expectancy, comorbidities, the presence of complications, and available resource and support systems (Figure 1).

The Elements of Decision Making Used to Determine Appropriate Efforts to Achieve Glycemic Targets.
Reproduced from Inzucchi SE et al. Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach. Diabetes Care Jun 2012;35(10):1364–1379, with permission from the American Diabetes Association.
Prof. Matthews explained the importance of striving for patient centrality, noting that patient involvement is much more crucial in chronic versus acute disease due to the priority for self-care. He stressed that it improves compliance and is more cost effective.
Making a Difference
Despite its departure from the more traditional, algorithm-based guideline, there are no guarantees that the new position statement will do anything more than generate a wide range of opinions and emotions among those in the medical community [Cefalu WT. Diabetes Care 2012]. Amanda Adler, MD, PhD, Institute of Metabolic Sciences, Cambridge, United Kingdom, discussed the guidelines' strengths, areas for future improvement, whether they will make a clinical difference, and what is next.
Among the position statement's strong points, Prof. Adler noted the enormous amount of work that went into creating it—more than 45 revisions between 2010 and 2012 [Cefalu WT. Diabetes Care 2012]—and described its recommendations as thoughtful and sensible. She agreed with the need for quality-of-life research and trials that deliver meaningful data on meaningful outcomes, and acknowledged the challenge of offering therapies to patients with multiple morbidities.
Prof. Adler said that many factors—pro and con—will determine whether the guidelines affect actual practice. On the con side, there is a lack of evidence that a patient-centered approach leads to better health, the fact that the ADA already calls for <7.0% HbA1C in most (but not all) patients, and the fact that the recommendations differ from others that people might prefer.
The new guidelines stand the greatest chance of promoting change if they inspire further research, and are understood, read, discussed, and disseminated; included in quality-improvement activities; easy to remember; applied where clinicians lack the latest information; and developed by influential, successful people who are widely admired.
According to Prof. Adler, the next round of guidance needs to be more inclusive, transparent, and evidence-based. In the interim, the goals of the ADA/EASD guidelines are to inspire clinicians to think about and choose treatment targets and strategies that best serve their patients. “Aspiring to this is unquestionably good,” she said.
The Changing Role of Drugs
Silvio E. Inzucchi, MD, Yale University, New Haven, Connecticut, USA, discussed the role of drugs in the management of hyperglycemia and related questions addressed in the new guidelines. He focused on the best drug to initiate therapy, the next steps if glucose is inadequately controlled, whether there is an optimal sequence of medications, when insulin should be used, and what patient features should guide therapy.
The burden of treatment for many people with complex chronic comorbidities must be acknowledged in the development of any treatment program; the clinician must weigh the benefits and risks of each therapy, especially in older patients who are managing multiple clinical conditions. Prioritizing from the patient's perspective is important [May C et al. BMJ 2009].
Given the increase in the number of medications for T2DM, clinicians and patients need information about their effectiveness and safety to make informed choices [Bennett WL et al. Ann Intern Med 2011]. Dr. Inzucchi explained that each drug class has a unique mechanism of action and lowers blood glucose to about the same extent. Many drugs have additional benefits, but their long-term effects are unknown. Moreover, there are major differences in side effects and costs (Table 1).
Properties of Anti-hyperglycemic Agents.
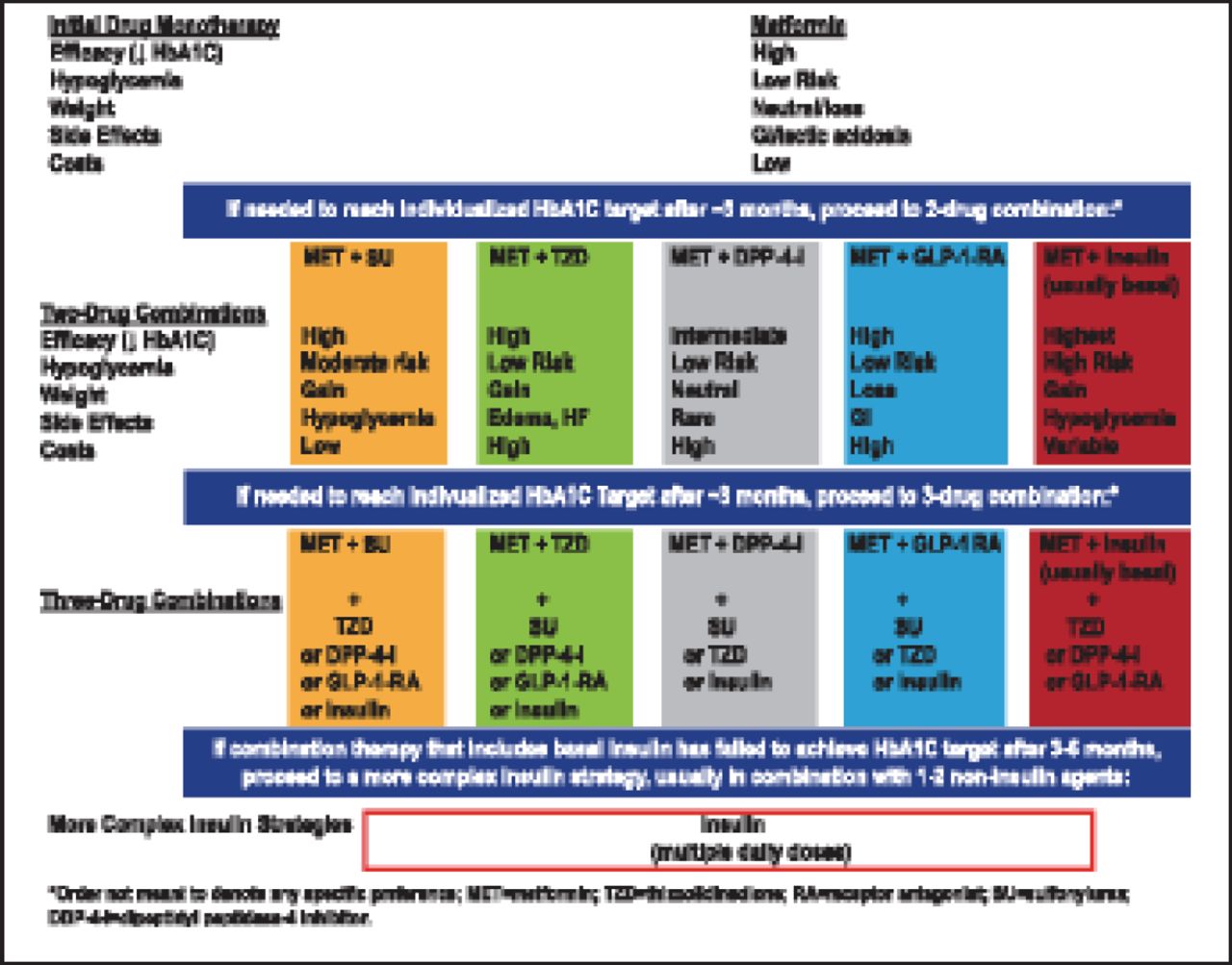
According to Dr. Inzucchi, glycemic targets and blood glucose-lowering therapies must be individualized. Diet, exercise, and education are the foundation of any T2DM therapy program. Unless contraindicated, metformin is the optimal first-line drug; however, more data are limited. Nonetheless, combination therapy with 1 to 2 other oral/injectable agents that minimize side effects is reasonable. Ultimately, many patients will require insulin therapy alone or in combination with other agents to maintain blood glucose (Figure 2).

Antihyperglycemic Therapy.
Reproduced from Inzucchi SE et al. Management of Hyperglycemiain Type 2 Diabetes: A Patient-Centered Approach. Diabetes Care Jun 2012;35(10):1364–1379, with permission from the American Diabetes Association.
Earlier guidelines focused drug treatment choices mainly on HbA1C levels after lifestyle modification [Robard H et al. Endocr Pract 2009]. For example, Nathan et al. [Diabetes Care 2008] recommended that clinicians check HbA1C levels every 3 months until <7.0%, then at least every 6 months thereafter, with new drug interventions whenever HbA1C levels reach ≥7.0%.
The new ADA/EASD guidelines shift the focus on medication choices from HbA1C levels alone and add patient-centered considerations. Dr. Inzucchi emphasized the need to make all treatment decisions in conjunction with patients (with a focus on their preferences, needs, and values) and stressed that comprehensive cardiovascular risk reduction should be a major focus of therapy.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.