

Summary
Diabetic peripheral neuropathy (DPN) affects up to 50% of patients with diabetes and is a major cause of morbidity and increased mortality. Its clinical manifestations, which include painful neuropathic symptoms and insensitivity, increase the risk for burns, injuries, and foot ulceration [Tesfaye S, Selvarajah D. Diabetes Metab Res Rev 2012]. This article discusses findings from recent studies on pharmaceutical agents used to treat DPN.
- Diabetes Mellitus
Diabetic peripheral neuropathy (DPN) affects up to 50% of patients with diabetes and is a major cause of morbidity and increased mortality. Its clinical manifestations, which include painful neuropathic symptoms and insensitivity, increase the risk for burns, injuries, and foot ulceration [Tesfaye S, Selvarajah D. Diabetes Metab Res Rev 2012]. Solomon Tesfaye, MD, University of Sheffield, Sheffield, United Kingdom, discussed findings from recent studies on pharmaceutical agents used to treat DPN.
Medication for diabetic peripheral neuropathic pain (DPNP) includes tricyclic antidepressants (TCAs), serotonin-norepinephrine reuptake inhibitors (SNRIs; eg, duloxetine), anticonvulsants (eg, pregabalin), opiates, membrane stabilizers, the antioxidant α-lipoic acid, and others. New agents that might have fewer side effects have emerged over the past 7 years [Tesfaye S, Selvarajah D. Diabetes Metab Res Rev 2012]. However, current treatments still provide suboptimal pain relief.
Questions about the management of DPNP center on the best first-line drug, the best combination of first-line drugs, whether to switch or combine various agents, the nature of a clinically meaningful response for monotherapy, length of time to determine efficacy, and whether to prescribe an early combination of drugs that work by different mechanisms versus a trial of maximum doses of monotherapy.
One study found that gabapentin and morphine combined achieve better analgesia at lower doses of each drug than either as a single agent, with constipation, sedation, and dry mouth being the most frequent adverse effects [Gilron I et al. N Engl J Med 2005]; another study reported that coadministration of prolonged-release oxycodone and existing gabapentin therapy has a clinically meaningful effect on DPNP [Hanna M et al. Eur J Pain 2008].
A randomized, double-blind, crossover trial compared the efficacy and safety of amitriptyline versus pregabalin in painful diabetic neuropathy. Pregabalin 150 mg BID was associated with fewer adverse effects than amitriptyline (Table 1) [Bansal D et al. Diabet Med 2009].
Amitriptyline Versus Pregabalin in DPNP.
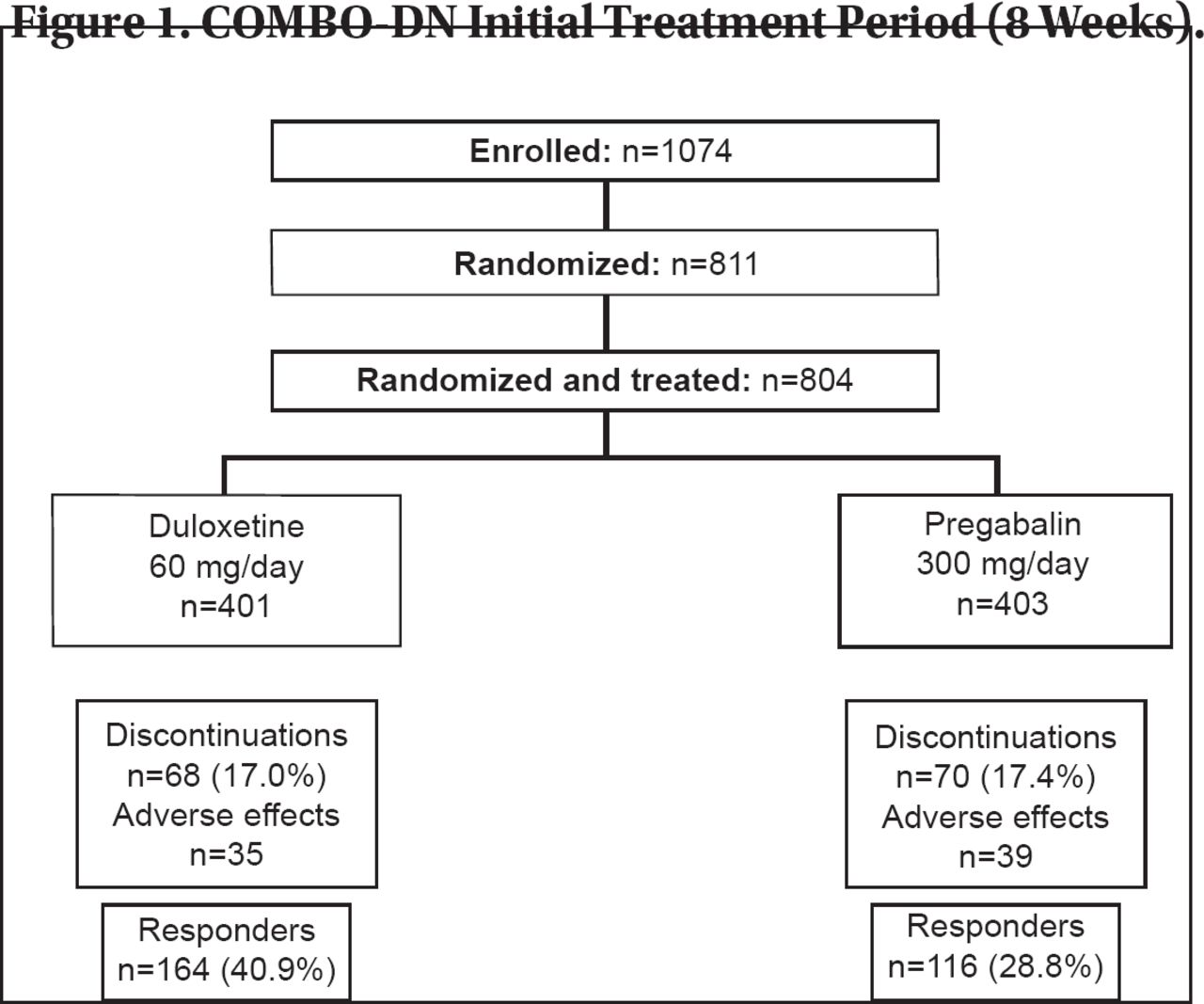
A Study in Painful Diabetic Neuropathy [COMBO-DN; Tesfaye S et al. Submitted; EUCTR 2009–010063–16-DE] was the largest double-blind randomized trial to date on combination treatment for DPNP. It investigated the efficacy of a combination treatment of duloxetine plus pregabalin compared with the maximal dose of each drug in monotherapy in patients with DPNP (Figure 1). As such, it addressed a common clinical question: Is it better to increase the dose of the current monotherapy or combine both treatments early in patients who do not respond to standard doses of duloxetine or pregabalin?

COMBO-DN Initial Treatment Period (8 Weeks).
Reproduced with permission from S. Tesfaye, MD.
The trial did not clearly demonstrate that standard dose combination therapy of duloxetine with pregabalin provides significantly better pain relief compared with high-dose monotherapy of either drug in DPNP patients with insufficient pain relief. There was no evidence that safety and tolerability are negatively affected when duloxetine is combined with pregabalin in these patients. For initial treatment, duloxetine (60 mg/day) provided
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.