

Summary
After completing a randomized controlled trial to examine the impact of a population-based diabetes screening program on mortality in England, it was concluded that screening for diabetes was not associated with a reduction in mortality and that the benefits of screening may be limited to those with detectable disease.
- Diabetes Mellitus
- Diabetes & Endocrinology Clinical Trials
- Nursing
- Diabetes & Metabolic Syndrome
After completing a randomized controlled trial to examine the impact of a population-based diabetes screening program on mortality in England, Rebecca K. Simmons, PhD, Medical Research Council Epidemiology Unit, Cambridge, United Kingdom, concluded that screening for diabetes was not associated with a reduction in mortality and that the benefits of screening may be limited to those with detectable disease.
Although modeling studies suggest that screening might reduce diabetes-related mortality by 26% to 40% if conducted among middle-aged adults every 3 to 5 years, there was no evidence from randomized trials to confirm if these estimates are correct. The ADDITION-Cambridge cluster-randomized controlled trial was conducted to assess the impact of a population-based screening program on mortality among people at high risk of undiagnosed diabetes [Simmons RK et al. Lancet 2012]. The study population comprised 20,184 individuals aged 40 to 69 years, from 32 general practices in Eastern England, who were considered to be at high risk of diabetes based on a validated risk score that included age, sex, body mass index (BMI), and prescription of antihypertensive medication or steroids as criteria. Twenty-seven practices were cluster randomized to a screening group (comprised of 16,047 individuals) and 5 practices to a no-screening control group (4137 individuals). Both the patients and practitioners in the no-screening group were unaware of the patients' high-risk status. All participants were tagged for mortality at the Office for National Statistics and followed for 10 years. Screening included random capillary blood glucose and HbA1C tests, a fasting capillary test, and a confirmatory oral glucose tolerance test. The primary analysis was a comparison of all-cause mortality rates and cardiovascular, cancer, and diabetes-related mortality rates between the screening and control groups. Analysis was by intention to screen accounting for clustering.
Baseline practice characteristics (list size, mean diabetes prevalence, and mean index of multiple deprivation score) were similar between screening and no-screening groups. Mean age (58 years), percentage of male participants (64%), BMI (30.5 kg/m2), and prescribed antihypertensives (45%) were also similar between groups.
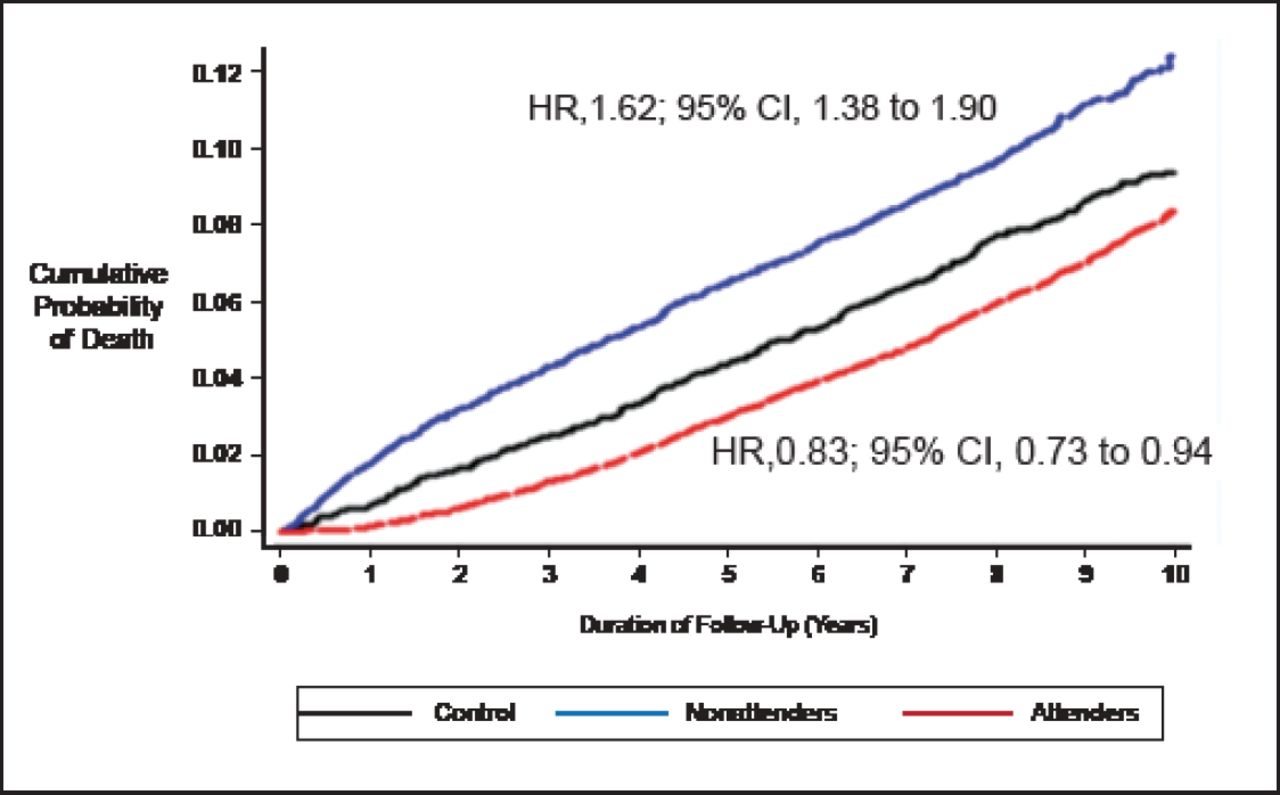
Over a median of 9.6 years of follow-up, 15,089 (94%) of the 16,047 high-risk individuals in screening practices were invited for screening. In all, 11,737 (73.1%) attended and 466 (2.9%) were diagnosed with diabetes. A total of 4137 individuals were followed in the no-screening practices. There were no differences in mortality rates by study group (Table 1). The difference in the cumulative incidence of death between the groups over time was not significant (HR, 1.06; 95% CI, 0.90 to 1.25; p=0.46). Compared with the control group, screening attenders had lower mortality (HR, 0.83; 95% CI, 0.73 to 0.94) and non-attenders had a higher mortality (HR, 1.62; 95% CI, 1.38 to 1.90; Figure 1).
Mortality Rate by Study Group.

Cumulative Incidence of Death in Attenders, Nonattenders, and No-Screening Control Group.
Reproduce with permission from R. Simmons, PhD.
The investigators concluded that the benefits of screening for diabetes may have been overestimated and restricted to those found to have diabetes and treated early. The benefits of screening might be improved by the detection and management of related cardiovascular risk factors alongside assessment of diabetes risk, repeated rounds of screening, and the identification of non-attenders and strategies to maximize their utilization of screening.
- © 2012 MD Conference Express®
Further Reading
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.