

Summary
Insulin glargine used to target normal fasting glucose for more than 6 years had a neutral effect on cardiovascular (CV) outcomes and cancers in high-risk patients with impaired fasting glucose (IFG), impaired glucose tolerance (IGT), or early diabetes. Although it reduced new onset diabetes, insulin glargine also increased hypoglycemia and modestly increased weight in the Outcome Reduction with Initial Glargine Intervention Trial [ORIGIN Trial Investigators. N Engl J Med 2012]. In the same trial, daily supplementation with n-3 fatty acids did not reduce CV events.
- Insulin Diabetes Mellitus
- Diabetes & Endocrinology Clinical Trials
- Hyperglycemia/Hypoglycemia
Insulin glargine used to target normal fasting glucose for more than 6 years had a neutral effect on cardiovascular (CV) outcomes and cancers in high-risk patients with impaired fasting glucose (IFG), impaired glucose tolerance (IGT), or early diabetes. Although it reduced new onset diabetes, insulin glargine also increased hypoglycemia and modestly increased weight in the Outcome Reduction with Initial Glargine Intervention Trial [ORIGIN Trial Investigators. N Engl J Med 2012]. In the same trial, daily supplementation with n-3 fatty acids did not reduce CV events. Hertzel C. Gerstein, MD, MSc, McMaster University and Hamilton Health Sciences, Hamilton, Ontario, Canada, reported the main results from the study.
The international double-blind trial with a 2×2 factorial design included 12,537 patients with diabetes (88%) or with IFG and/or IGT but no diabetes (12%) randomized to receive insulin glargine (with a target fasting blood glucose level of ≤95 mg/dL) or standard care. Participants also received a 1-g capsule containing at least 900 mg (90% or more) of ethyl esters of n-3 fatty acids or placebo daily. The coprimary outcomes of the insulin glargine versus standard care arm were nonfatal myocardial infarction, nonfatal stroke, or death from CV causes, and these events plus revascularization or hospitalization for heart failure. Microvascular outcomes, incident diabetes, hypoglycemia, weight gain, and cancers were also compared between the two groups. The primary outcome in the n-3 fatty acids arm was death from CV causes. The median follow-up was 6.2 years.
Rates of incident CV outcomes were similar in the glargine and the standard care groups: 2.94 and 2.85 per 100 person-years, respectively, for the first coprimary outcome (MI, stroke, or CV death; HR, 1.02; 95% CI, 0.94 to 1.11; p=0.63) and 5.52 and 5.28 per 100 person-years, respectively, for the second coprimary outcome (MI, stroke, CV death, revascularization, heart failure; HR, 1.04; 95% CI, 0.97 to 1.11; p=0.27). Differences in the incidence of any cancer were not significant (HR, 1.00; 95% CI, 0.88 to 1.13; p=0.97).
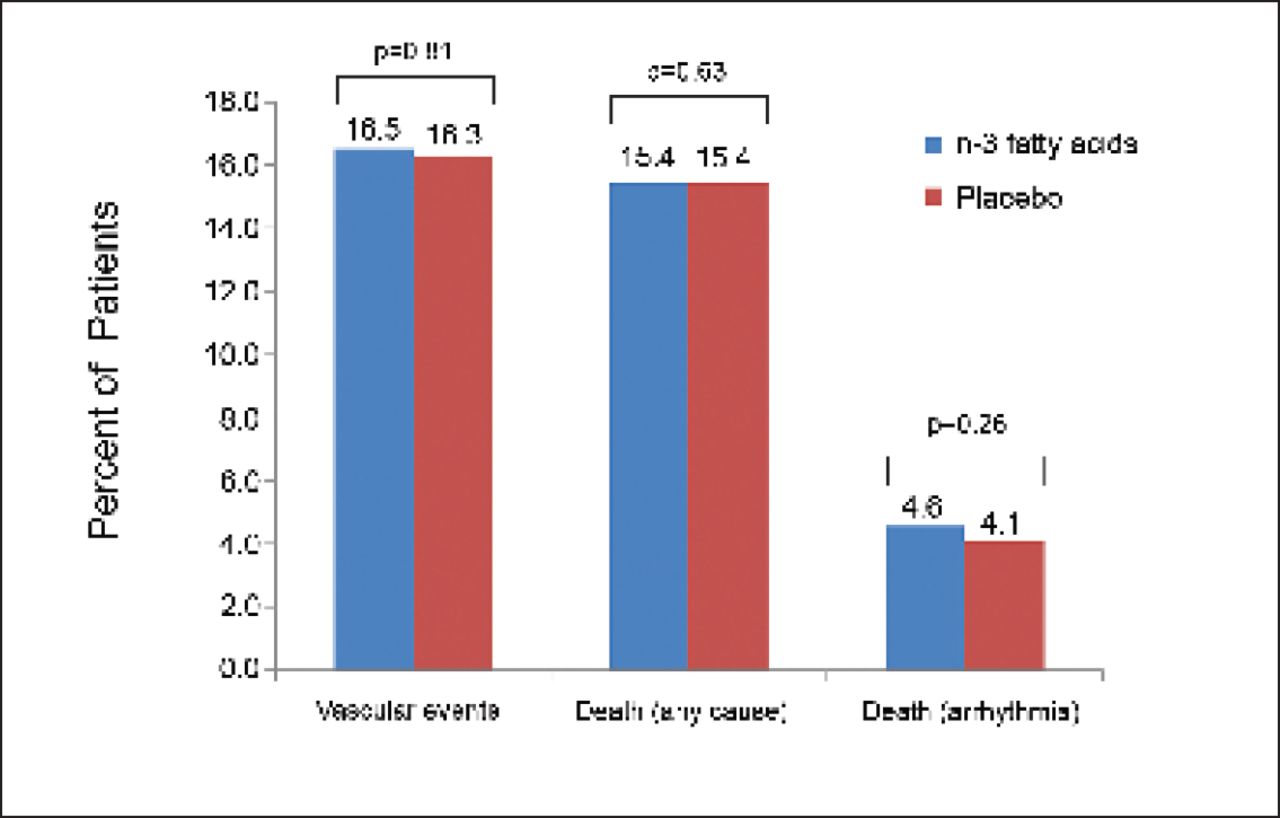
Among patients receiving n-3 fatty acids versus placebo, the incidence of primary outcome was not significantly decreased (574 patients [19.1%] vs 581 patients [9.3%]; HR, 0.98; 95% CI, 0.87 to 1.10; p=0.72). The use of n-3 fatty acids also had no significant effect on the rates of major vascular events (1034 patients vs 1017 patients; HR, 1.01; 95% CI, 0.93 to 1.10; p=0.81), death from any cause (951 vs 964; HR, 0.98; 95% CI, 0.89 to 1.07; p=0.63), or death from arrhythmia (288 vs 259; HR, 1.10; 95% CI, 0.93 to 1.30; p=0.26; Figure 1). Triglyceride levels were reduced by 14.5 mg/dL more among patients receiving n-3 fatty acids versus placebo (p<0.001), without a significant effect on other lipids. Adverse effects were similar in the two groups [ORIGIN Trial Investigators. N Engl J Med 2012].

Event Rates.
Matthew C. Riddle, MD, Oregon Health & Science University, Portland, Oregon, USA, presented new ORIGIN trial subgroup data. The findings indicate that target-directed intervention early in dysglycemia can maintain baseline HbA1C levels for at least 5 years and that the glargine-based regimen is more likely to keep HbA1C <6.5% than standard care.
The main independent predictors of maintaining mean HbA1C <6.5% up to 5 years were type 2 diabetes versus no type 2 diabetes, baseline HbA1C per 1%, alcohol use >2 times/week, and glargine versus standard treatment (p<0.001 for all).
The data showed that <50% of diabetic patients had HbA1C levels <6.5% at baseline, but this figure rose to 60% at 5 years among those randomized to glargine and dropped to 45% among those on standard therapy. In the group without diabetes, 91% of patients had baseline HbA1C levels <6.5%. This number fell to 87% at 5 years in those randomized to glargine and to 79% at 5 years among those on standard therapy.
Both titrated glargine and a standard care approach kept HbA1C levels near baseline values for at least 5 years. According to Dr. Riddle, more data and further analyses are needed to define the benefits versus the risks of the two approaches.
For more information, please see the MD Conference Express review of the ORIGIN presentation in our ADA Report.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.