

Summary
Newer antiplatelet agents offer greater consistency and protection than the current standard of care. This article discusses the latest antiplatelet therapy for percutaneous coronary intervention.
- Myocardial Infarction
- Thrombotic Disorders
- Cardiology
- Interventional Techniques & Devices
Newer antiplatelet agents offer greater consistency and protection than the current standard of care. Eyas Al-Mousa, MD, Jordan University Hospital, Amman, Jordan, discussed the latest antiplatelet therapy for percutaneous coronary intervention (PCI).
Antiplatelet therapy is the cornerstone of treatment for patients who have acute coronary syndromes (ACS) and/or are undergoing PCI [Angiolillo DJ et al. J Am Coll Cardiol 2007]. In the last 2 decades, dual antiplatelet therapy with clopidogrel and acetylsalicylic acid has become the standard of care for patients with ACS.
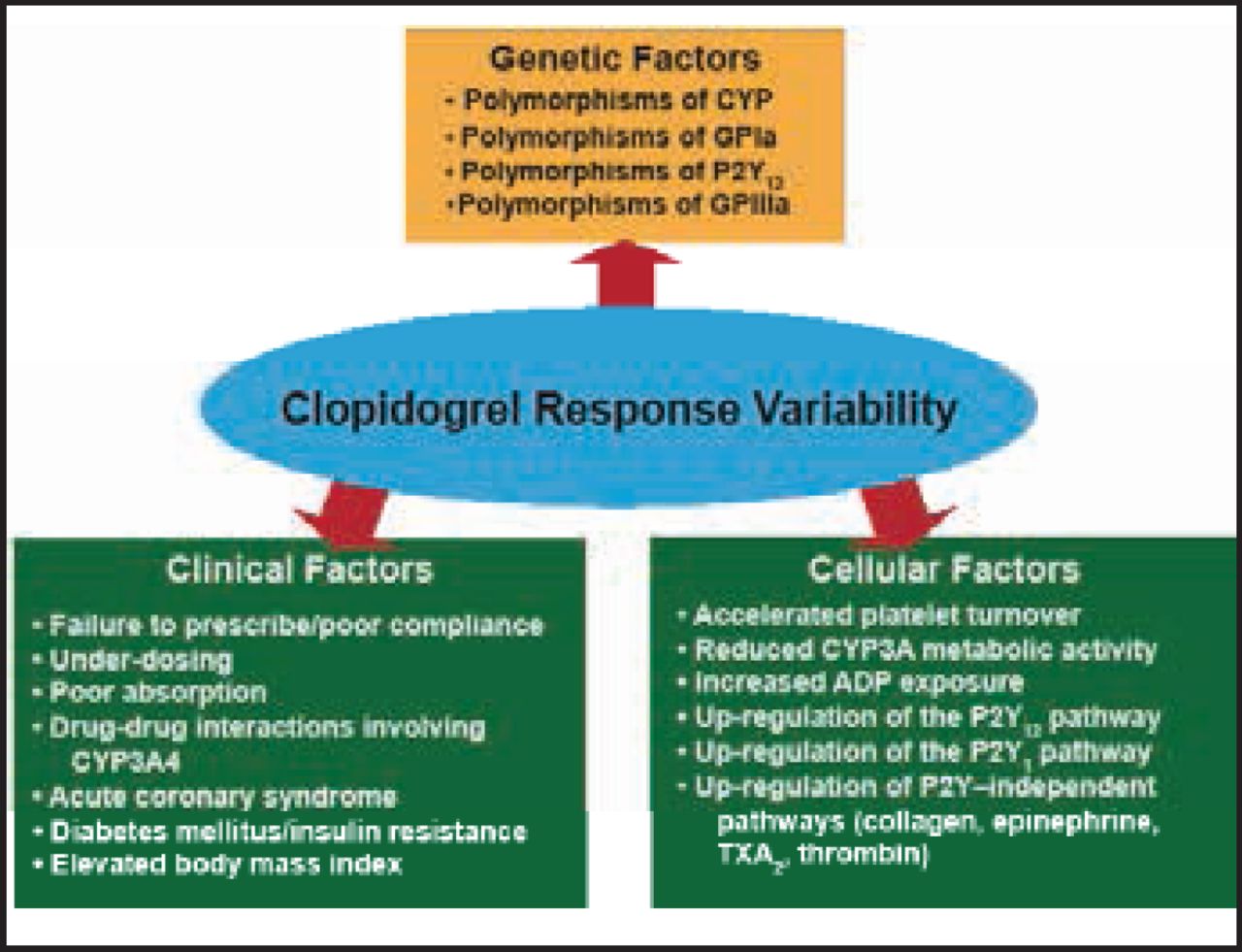
However, clopidogrel has drawbacks that include delayed therapeutic effect, significant interindividual variability of platelet aggregation inhibition or reduced action on thrombocytes due to interaction with other drugs or genetic polymorphisms. Although aspirin enhances the effects of clopidogrel, numerous in vitro studies have still verified that individual responsiveness to clopidogrel is not uniform in all patients and varies in response to genetic, clinical, and cellular factors (Figure 1) [Angiolillo DJ et al. J Am Coll Cardiol 2007].

Clopidogrel Response Variability.
ADP=adenosine diphosphate; CYP=cytochrome P450; GP=glycoprotein.
Reprinted from Am J Cardiol, Vol 101/4, Angiolillo DJ et al. Functional effects of high clopidogrel maintenance dosing in patients with inadequate platelet inhibition on standard dose treatment, 440–5, Copyright 2008, with permission from Elsevier.
Prasugrel, which represents the third generation of thienopyridines, inhibits platelet aggregation by irreversibly blocking the adenosine diphosphate P2Y12 receptor. In a randomized trial that compared prasugrel and clopidogrel loading doses (LDs) on rate of onset, magnitude, and consistency of platelet inhibition, Brandt et al. [Am Heart J 2007] found that a 60-mg LD of prasugrel resulted in more rapid (p<0.001), potent (p<0.001), and consistent (p<0.01) inhibition of platelet function than a 300-mg LD of clopidogrel. In the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel-Thrombolysis in Myocardial Infarction [TRITON-TIMI] 38, treatment with prasugrel compared with clopidogrel resulted in a significantly lower rate of ischemic events (HR, 0.81; 95% CI, 0.73 to 0.90; p<0.001) [Wiviott S et al. N Engl J Med 2007].
Ticagrelor is an oral, reversible, direct-acting inhibitor of the adenosine diphosphate receptor P2Y12 that has a more rapid onset and more pronounced platelet inhibition than clopidogrel [Wallentin L et al. N Engl J Med 2009]. The Platelet Inhibition and Patient Outcomes [PLATO] trial demonstrated that treatment with ticagrelor versus clopidogrel in a broad population of patients with ACS substantially reduced the primary composite endpoint of death, myocardial infarction, or stroke by 16% (95% CI, 8 to 21), as well as the rates of all-cause death and death from vascular causes [Wallentin L et al. N Engl J Med 2009].
According to Prof. Al-Mousa, 1000 ACS patients using ticagrelor versus clopidogrel for 12 months resulted in 14 fewer deaths, 11 fewer myocardial infarctions, and 7 fewer cases with stent thrombosis, with no increase in bleedings requiring transfusion. “Platelets are the principal effectors of hemostasis and key mediators in the pathogenesis of thrombosis. With clopidogrel, a wide response variability may exist and a substantial percentage of patients can exhibit nonresponsiveness,” he explained.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.