

Summary
Globally, pulmonary vascular disease associated with congenital heart disease (CHD) may be the most preventable cause of pulmonary artery hypertension and related mortality and morbidity [Adatia I et al. Chest 2010]. This article presents an overview of advanced and combination therapies in patients with pulmonary arterial hypertension-CHD.
- Hypertensive Disease
- Cardiology
- Thromboembolic Disease
Globally, pulmonary vascular disease associated with congenital heart disease (CHD) may be the most preventable cause of pulmonary artery hypertension and related mortality and morbidity [Adatia I et al. Chest 2010]. Mohammed Omar Galal, MD, PhD, MBA, Prince Salman Heart Center, Riyadh, Saudi Arabia, presented an overview of advanced and combination therapies in patients with pulmonary arterial hypertension (PAH)-CHD.
Although progress in the diagnosis and treatment of CHD has reduced the number of PAH-CHD cases in Western nations, few PAH patients in developing countries have access to treatment. Adatia et al. [Chest 2010] estimate that 3 million children worldwide are at risk for the development of pulmonary vascular disease due to CHD; most have a reparable heart defect, such as an isolated atrial septum, ventricular septal defect, or patent ductus arteriosus.
PAH-CHD is classified into 4 types suitable for advanced therapy. These include 1) Eisenmenger Syndrome, 2) moderate to large shunt lesions with PAH, 3) small defects with PAH, and 4) PAH after repair of CHD [Galie N et al. Eur Heart J 2009; Simonneau G et al. J Am Coll Cardiol 2009]. Eisenmenger Syndrome is the most advanced form of pulmonary vascular disease secondary to CHD [Adatia I et al. Chest 2010].
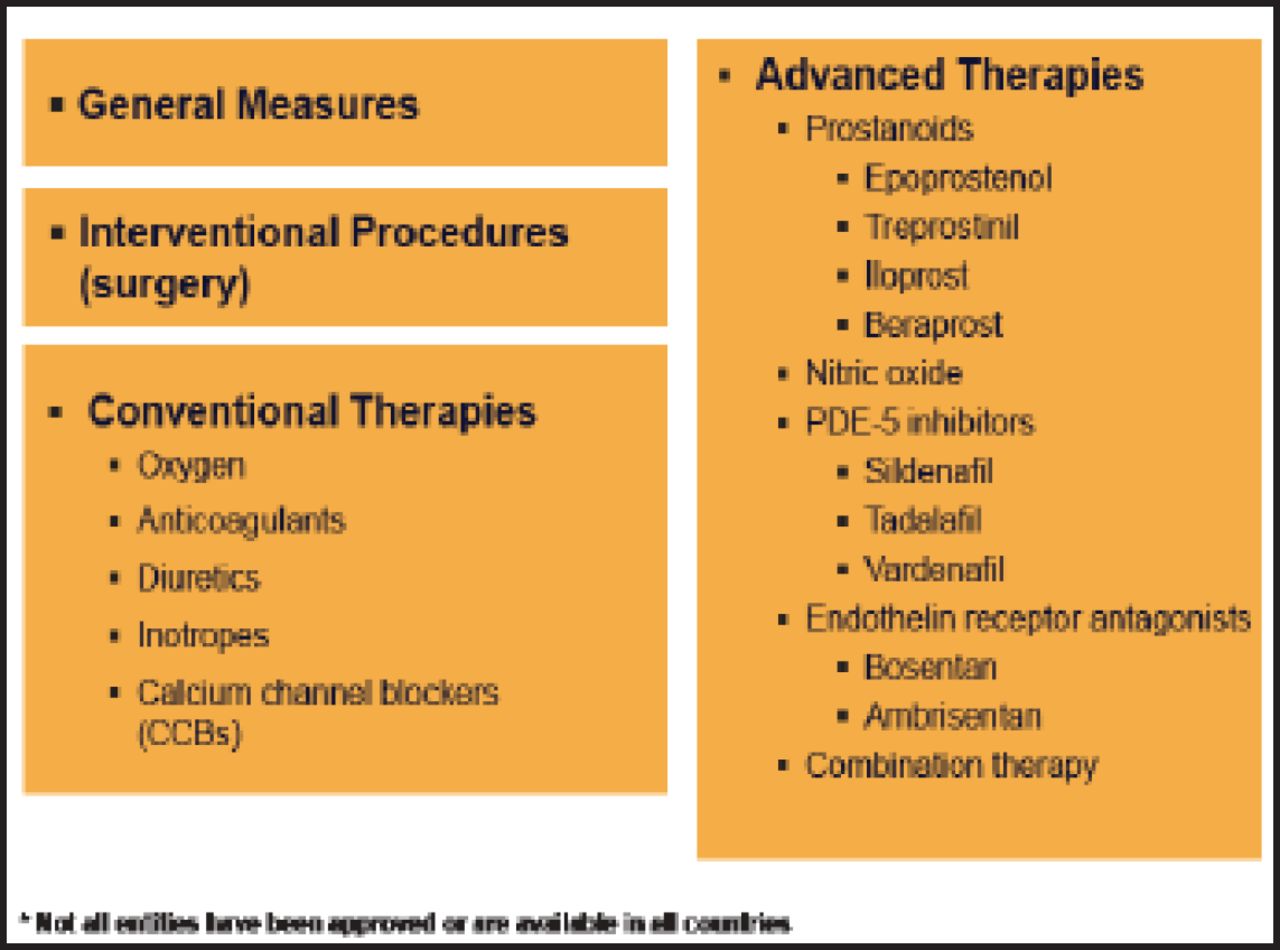
Treatment options in PAH range from general measures to advanced therapies (Figure 1). Conventional treatments include diuretics, anticoagulants, oxygen therapy, digoxin, and calcium channel blockers. In a randomized trial with 2 years of follow-up, Sandoval et al. [Am J Respir Crit Care Med 2001] found that nocturnal oxygen therapy did not modify the natural history of patients with advanced Eisenmenger Syndrome. Calcium channel blockers benefit around 10% of patients with PAH and seem to improve survival, said Prof. Galal.

Treatment Options in PAH*.
PAH=pulmonary arterial hypertension; PDE-5=phosphodiesterase 5.
According to Prof. Galal, advanced therapy should be used if there is a negative vasoreactivity test or lack of clinical improvement with calcium channel blockers. It can also be used in all groups with a NYHA functional class of II, III, or IV. However, most data on advanced care are based on studies with idiopathic PAH and PAH due to scleroderma, and the therapies are very expensive.
The 3 classes of advanced therapy include endothelin-1 receptor antagonists, phosphodiesterase 5 inhibitors, and prostanoids. Bosenten has been demonstrated to improve exercise capacity and stroke volume in patients without Down syndrome [Rubin LJ et al. N Engl J Med 2002]. In a medium-term follow-up study of adult patients with PAH associated with CHD, Duffels et al. [Congenit Heart Dis 2007] found that advanced treatment seemed to stabilize disease and decrease the rate of deterioration, especially in younger patients.
Based on these and other data, Prof. Galal concluded that PAH-CHD remains a serious disease leading to reduced quality of life and longevity, 4 classes of PAH-CHD justify advanced therapies, that short-term studies have confirmed the efficacy and safety of advanced/combination therapies, and long-term studies are still needed.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.