

Summary
Pandemic diabetes and cardiovascular disease have created an imperative to develop risk-prediction models for early identification of patients with undiagnosed type 2 diabetes or those at risk of developing the disease [Collins GS et al. BMC Medicine 2011]. This article discusses the current status of risk-assessment tools.
- Diabetes Mellitus
- Cardiometabolic Disorder
Pandemic diabetes and cardiovascular disease have created an imperative to develop risk-prediction models for early identification of patients with undiagnosed type 2 diabetes or those at risk of developing the disease [Collins GS et al. BMC Medicine 2011]. Nick Wareham, MBBS, PhD, Institute of Metabolic Science, Cambridge, United Kingdom, discussed the current status of risk-assessment tools.
A diabetes risk score is a prognostic model [Moons KG et al. BMJ 2009] that has public health and clinical implications. On the public health level, using a risk score to rank individuals can help target therapy at those at greatest risk and identify those who need more definitive testing. Clinically, risk scores can be used to estimate the likely absolute benefit from intervention and motivate behavior change.
According to Prof. Wareham, risk-prediction models vary in cumulative complexity from already-available information and add-in data from self-completed or assisted questionnaires to clinical measures (including biomarkers) and genetic findings.
A good risk score is usually defined as one that 1) accurately estimates an individual's risk, ie, predictions are based on a score that closely matches what is observed (calibration), 2) reliably distinguishes between high-risk people who will likely develop the condition and those at low risk who are less likely to do so (discrimination), and 3) performs well in new populations (generalizability) [Noble D et al. BMJ 2011].
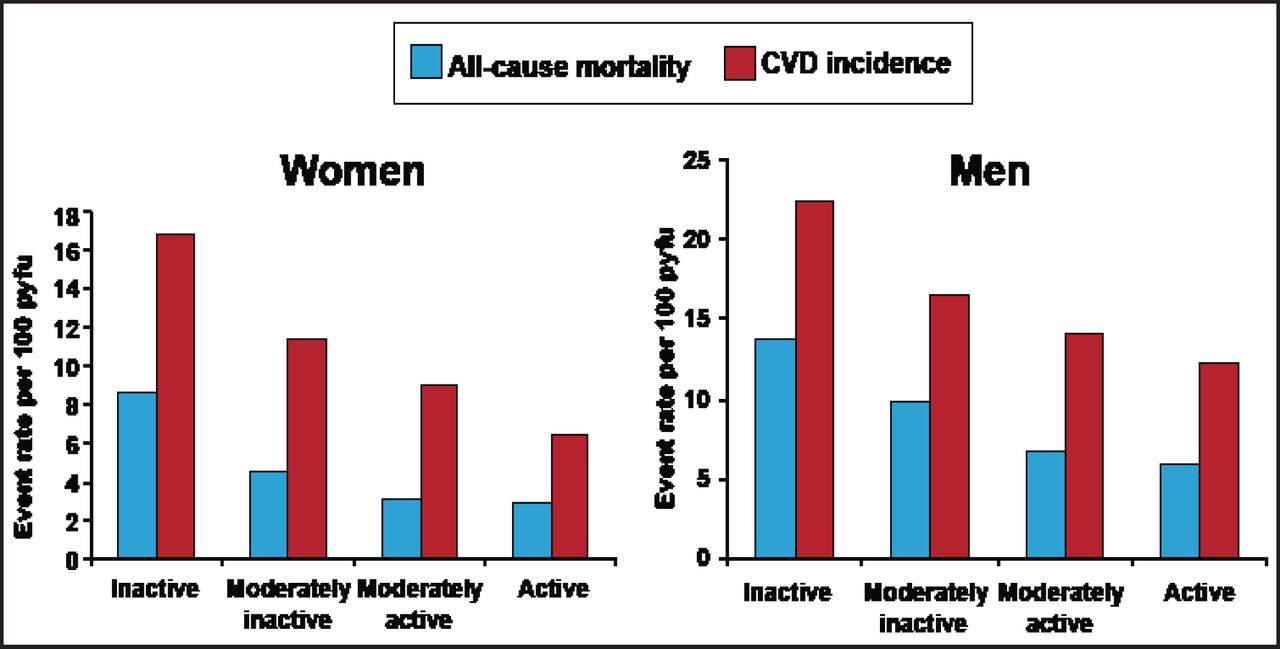
Griffin et al. [Diabetes Metab Res Rev 2000] found that a simple score, using only data routinely collected in general practice, can help identify those at risk of diabetes. Rahman et al. [Fam Pract 2008] demonstrated that a risk score comprised of only commonly collected nonbiochemical parameters could effectively identify those at risk of type 2 diabetes. Similarly, simple questions about leisure time and work-related physical activity that can be rapidly obtained by any physician at no cost can help estimate a patient's risk of coronary heart disease (Figure 1) [Arsenault BJ et al. Atherosclerosis 2010].

Relationship Between Activity Levels and Risk of All-Cause Mortality or Cardiovascular Event.
Reprinted from Khaw KT et al. Work and leisure time physical activity assessed using a simple, pragmatic, validated questionnaire and incident cardiovascular disease and all-cause mortality in men and women: The European Prospective Investigation into Cancer in Norfolk prospective population study. Int J Epidemiol. 2006;35(4):1034–43, by permission of Oxford University Press.
Salomaa et al. [PLoS One 2010] demonstrated that after taking obesity and other classic risk factors into account, several novel biomarkers (eg, adiponectin, apolipoprotein B, C-reactive protein, and ferritin) improve clinical prediction of type 2 diabetes. Recently, Forouhi et al. [Diabetologia 2012] found an inverse association between circulating 25-hydroxyvitamin D and incident type 2 diabetes; and Pfister et al. [PLoS Med 2011] reported evidence of a causal relationship between the B-type natriuretic peptide system and the etiology of type 2 diabetes.
Recent genome-wide association studies have identified many loci in type 2 diabetes pathophysiology and β-cell dysfunction [Manning AK et al. Nat Genet 2012]. Voight et al. [Nat Genet 2010] found 12 type 2 diabetes susceptibility loci identified through largescale association analysis, while Manning et al. [Nat Genet 2012] discovered 6 previously unknown loci related to fasting insulin at p<5×10(–8). Risk variants were associated with higher triglyceride and lower high-density lipoprotein-cholesterol levels, suggesting a role for these loci in insulin-resistance pathways.
The best approach for predicting incident type 2 diabetes depends how the information will be used, ie, for public health or clinical purposes. According to Prof. Wareham, routine data score is the most effective means of predicting performance from a population perspective. Clinically, he concluded that making patients aware of their risk can encourage them to take action to reduce it. In addition, a numerical presentation of risk instead of simple risk categories leads to more accurate risk perception and can influence treatment decisions. The relative risk-reduction format is the best way to encourage patients to accept treatment, while the number-needed-to-treat format is the least effective way to encourage acceptance of treatment.
He advised clinicians to ensure that their choice of instrument has been tested in the population in which it is to be used and to be aware of different methods of transmitting risk information to patients and their impact on patients.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.