

Summary
Ectopic fat is defined as storage of triglycerides in tissues other than adipose tissue, such as the liver, skeletal muscle, heart, and pancreas [Snel M et al. Int J Endocrinol 2012]. This article discusses ectopic fat accumulation and cardiometabolic risk.
- Cardiometabolic Disorder
- Obesity
Ectopic fat is defined as storage of triglycerides in tissues other than adipose tissue, such as the liver, skeletal muscle, heart, and pancreas [Snel M et al. Int J Endocrinol 2012]. Marja-Riitta Taskinen, MD, University of Helsinki, Helsinki, Finland, discussed ectopic fat accumulation and cardiometabolic risk.
Excess body adiposity, especially abdominal obesity and ectopic fat accumulation, is a key risk factor in the development of a number of chronic diseases [Thomas EL et al. Nutr Res Rev 2012]. It can interfere with cellular functions, and, hence, organ functions, and is associated with insulin resistance [Snel M et al. Int J Endocrinol 2012].
Adipose tissue dysfunction is largely characterized by large adipocytes and secretion of adipokines with a proinflammatory profile, ultimately leading to ectopic fat deposition (among others) [Blüher M. Exp Clin Endocrinol Diabetes 2009].
Although visceral fat accounts for only 10% to 15% of ectopic fat accumulation, 82% to 97% is stored as subcutaneous fat. Other major sites of ectopic fat accumulation include the heart (0% to 3%), the liver (5% to 30%), and skeletal muscle fat (10% to 15%).
Ectopic fat is an important predictor of metabolic (in particular, insulin resistance) and cardiovascular disease (CVD), carrying more risk than general fat accumulation. Recent studies have shown a link between ectopic fat accumulation, as cardiac (epicardial or intramyocardial fat) and/or visceral and/or hepatic fat, and development of atherosclerosis, coronary heart disease, and hypertension (Figure 1) [Gastaldelli A, Basta G. Nutr Metab Cardiovasc Dis 2010].

Ectopic Fat and Cardiometabolic Risk.
Reprinted from Nutr Metab Cardiovasc Dis, Vol 20/7, Gastaldelli A & Basta G, Ectopic fat and cardiovascular disease: What is the link?, 481–90, Copyright (2010), with permission from Elsevier.
According to Dr. Taskinen, fatty liver produces a plethora of risk factors for CVD. The mediators that may link it and CVD include glucose, very low-density lipoprotein (VLDL), high-density lipoprotein (HDL), alanine aminotransferase and aspartate aminotransferase, fibrinogen, factor VII and plasminogen activator inhibitor-1, angiotensinogen, C-reactive protein and serum amyloid A, and tumor necrosis factor-α and interleukin-6. The atherogenic lipoprotein triad (increased large VLDL, increased small dense LDL, and decreased HDL-C) and hepatic steatosis lead to an increased risk of coronary artery disease.
Although obesity increases the risk of CVD and premature death, not all obese people (20% to 30%) develop the metabolic abnormalities associated with obesity [Taskinen MR et al. Arterioscler Thromb Vasc Biol 2011]. In those who do, nonalcoholic fatty liver disease, especially in its more severe forms, is linked to an increased risk of CVD, independent of underlying cardiometabolic risk factors [Stefan N et al. Endocr Rev 2008; Gastaldelli A et al. Hepatology 2009; Speliotes EK et al. Hepatology 2010].
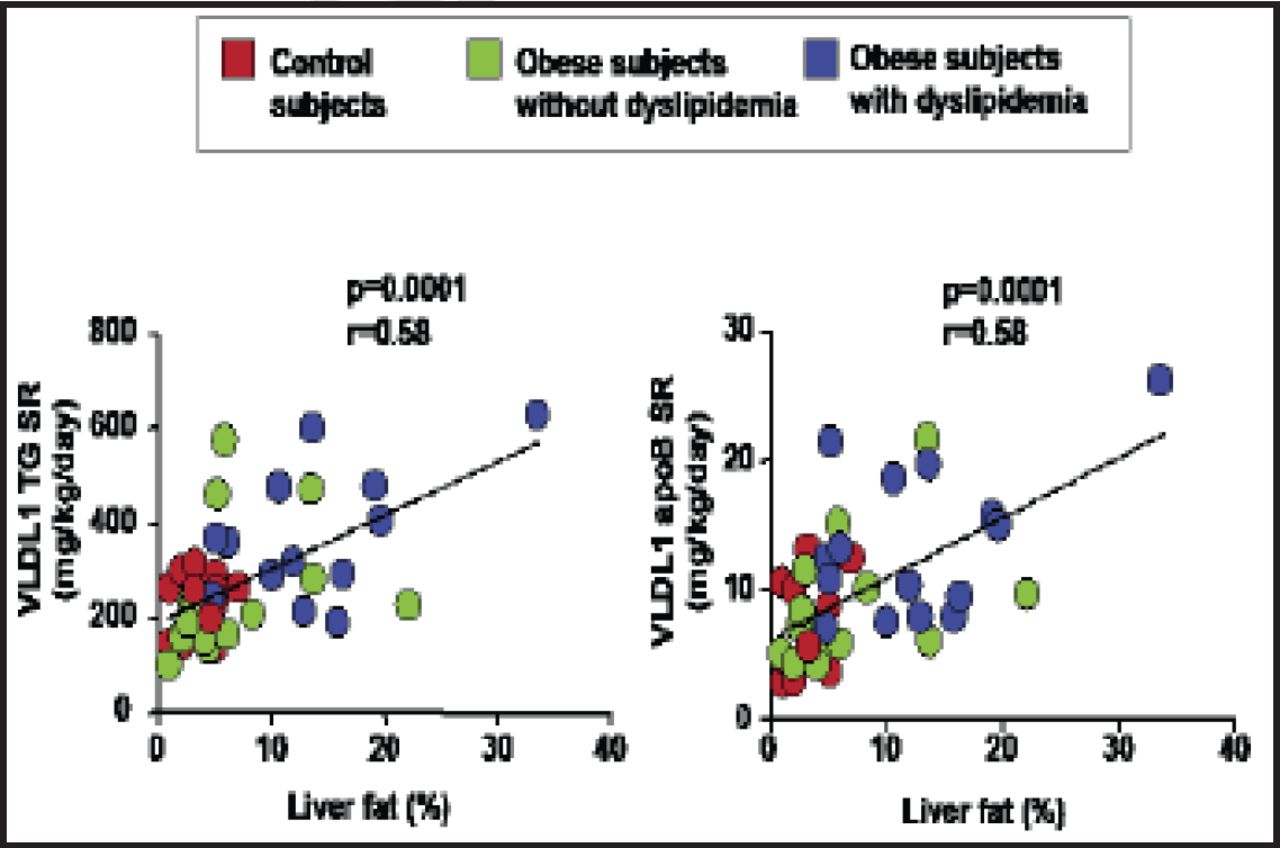
Taskinen and colleagues investigated if hypertriglyceridemia (HTG) in obese men with similar body mass indexes, waist circumferences, and levels of visceral adiposity is caused by increased hepatic secretion induced by increased liver fat. Results showed that dual metabolic defects are required to produce HTG in obese subjects with similar levels of visceral adiposity, ie, the combination of increased secretion driven by liver fat content and severely impaired clearance of triglyceride-rich VLDL1 particles linked to the elevation of apolipoprotein CIII. Notably, there was an overproduction of large VLDL particles associated with small dense LDL and lowering of HDL as seen in the atherogenic lipid triad. The data suggest that overproduction of VLDL particles is a mechanism to export extra fat out of the liver (Figure 2) [Taskinen MR et al. Arterioscler Thromb Vasc Biol 2011]. The data highlights the clinical importance of assessing hypertriglyceridemic waist to indentify obese subjects at high cardiometabolic risk.

Liver Fat Drives Production of VLDL1.
Reproduced with permission from MR Taskinen, MD.
Strategies that decrease liver fat and improve insulin sensitivity may boost whole-body insulin sensitivity [Byrne CD. Diabet Med 2012] and reduce CVD risk factors and lipotoxicity related to contractile, mitochondrial, and endoplasmic reticulum dysfunction; steatosis; and apoptosis [Wende AR, Abel ED. Biochim Biophys Acta 2010].
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.