

Summary
Cardiac resynchronization therapy (CRT) improves mortality and morbidity in heart failure patients with depressed ejection fraction and wide QRS complex, but response varies, with about one third of CRT recipients failing to improve. The Speckle Tracking-Assisted Resynchronization Therapy for Electrode Region trial [STARTER] tested the hypothesis that echo-guided left ventricular (LV) lead placement that targets the site of latest LV mechanical activation is superior to routine positioning for CRT.
- Interventional Techniques & Devices Clinical Trials
- Heart Failure
Cardiac resynchronization therapy (CRT) improves mortality and morbidity in heart failure (HF) patients with depressed ejection fraction (EF) and wide QRS complex, but response varies, with about one third of CRT recipients failing to improve. The Speckle Tracking-Assisted Resynchronization Therapy for Electrode Region trial [STARTER] tested the hypothesis that echo-guided left ventricular (LV) lead placement that targets the site of latest LV mechanical activation is superior to routine positioning for CRT. Samir Saba, MD, University of Pittsburgh, Pittsburgh, Pennsylvania, USA, reported findings from the trial.
A total of 187 patients with New York Heart Association Classes II-IV HF who were eligible for CRT, based on LVEF and QRS-duration criteria, were randomly assigned to device implantation with lead placement that was guided or not guided by speckle-tracking echocardiography. In each case, the site of latest mechanical activation was determined by assessing the time to peak radial strain that was associated with myocardial wall thickening. The primary endpoint was a composite of death or HF hospitalization.
Investigators found no significant difference in procedural or fluoroscopic times between the echo-guided and routine strategies. A higher rate (30%) of exact concordance of the LV lead with the site of latest mechanical activation was achieved in the echo-guided group compared with 12% (p=0.006) that occurred fortuitously in the group that was not guided by echocardiography (routine practice). Echo-guided placement was at the exact myocardial target or adjacent to it in 85% of patients in the echo-guided group versus 66% of those in the routine group (p=0.009).
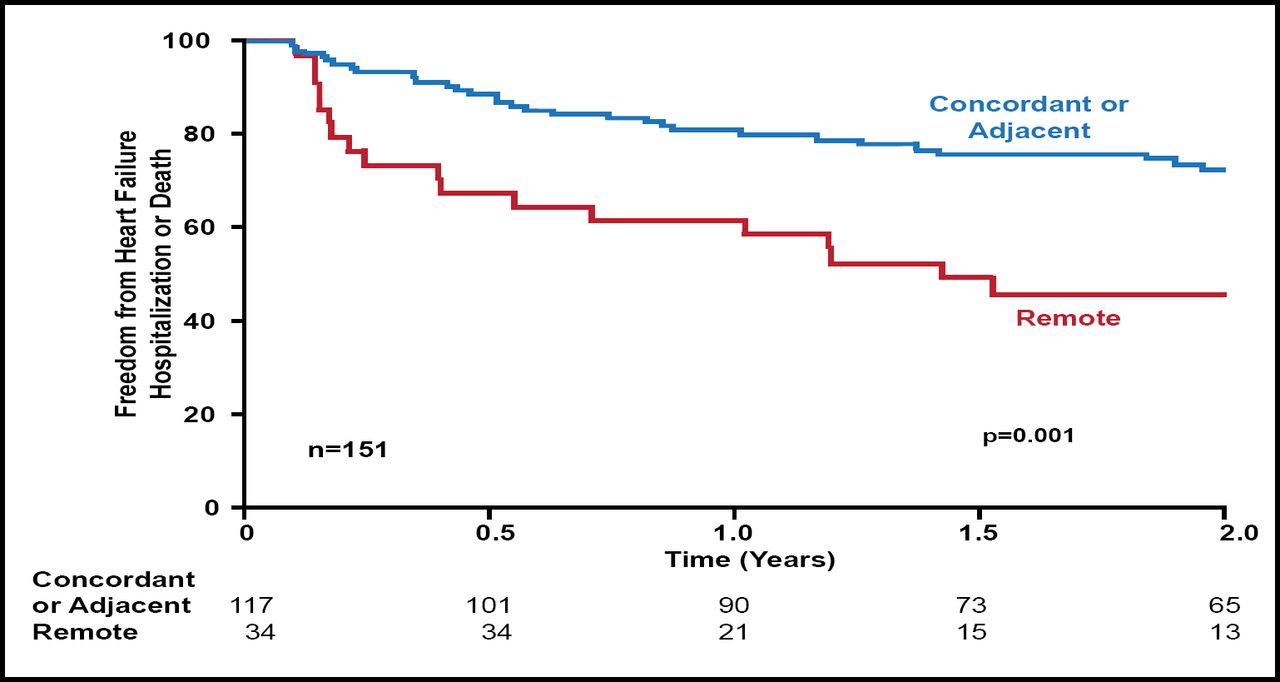
Over 2 years of follow-up, the intention-to-treat primary endpoint of death or HF hospitalization was significantly lower in the echo-guided group compared with the routine LV lead positioning group (p=0.006). Rates of HF hospitalization or death were also significantly lower in the concordant or adjacent LV lead placement group versus remote positioning (p=0.001; Figure 1). The incidence of death or the need for transplant or LV assist device was significantly lower among patients with concordant or adjacent versus remote LV lead positioning (p=0.002).

HF Hospitalization or Death over Time by Echo-Guided or Routine Left Ventricular Lead Position.
Reproduced with permission from S. Saba, MD.
In the STARTER trial, exact or adjacent concordance to the site of latest mechanical activation, as defined by speckle-tracking echocardiography, improved outcomes, including death/HF hospitalization-free survival and LV reverse remodeling and EF. Investigators concluded that a strategy of echo-guided LV lead delivery at or adjacent to the latest mechanical activation site is superior to unguided LV lead placement, as it improves patients' response to CRT.
- © 2012 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.