

Summary
This article discusses the complexities of determining which heart failure patients benefit from an implantable cardioverter-defibrillator.
- Interventional Techniques & Devices
- Heart Failure Guidelines
Primary Prevention ICDs for Heart Failure
Andrew E. Epstein, MD, University of Pennsylvania, Philadelphia, Pennsylvania, USA, discussed the complexities of determining which heart failure (HF) patients benefit from an implantable cardioverter-defibrillator (ICD). According to the American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines, patients with HF should wait at least 40 days post myocardial infarction (MI) to receive an ICD. The Defibrillator in Acute Myocardial Infarction Trial [DINAMIT; Hohnloser SH et al. N Engl J Med 2004] and the Immediate Risk Stratification Improves Survival study [IRIS; Steinbeck G et al. N Engl J Med 2009] reported no difference in overall mortality between HF patients with low left ventricular ejection fraction (LVEF) who were treated with ICDs versus optimal medical therapy (OMT) within 40 days post MI. In DINAMIT, more control patients died from arrhythmia versus ICD patients (p=0.009), while more ICD patients died from nonarrhythmic causes (p=0.02).
The Valsartan in Acute Myocardial Infarction Trial [VALIANT; Pfeffer A et al. N Engl J Med 2003] reported that patients had the highest risk of sudden death or cardiac arrest in the first 30 days after having an MI (1.4%/month). The Multicenter Automatic Defibrillator Implantation Trial II [MADIT-II; Moss A et al. N Engl J Med 2002] reported improved survival in patients who received ICDs versus those who received conventional therapy from 9 months to 3 years (p=0.007). Patients in this study with an implanted ICD had absolute reductions in mortality of 12% at 1 year, 28% at 2 years, and 28% at 3 years compared with patients who received conventional therapy. In the Multicenter Automatic Defibrillator Implantation With Cardiac Resynchronization Therapy trial [MADIT-CRT; Zareba W et al. Circulation 2011], cardiac resynchronization plus ICD (CRT-D) was associated with a 34% reduction in relative risk of an HF event. Patients with left bundle branch block (LBBB) received substantial benefits from CRT-D, but patients without an LBBB did not. In the the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction trial [REVERSE; Daubert C et al. J Am Coll Cardiol 2009], among patients with shorter baseline QRS width (120 to 138 ms), the clinical composite score had worsened at 12 months in 27% of patients with CRT-On versus 18% of patients with CRT-Off. The percentage of patients with longer QRS widths who worsened at 12 months with CRT-On versus CRT-Off were QRS width 139 to 152 ms (14% vs 23%), QRS width 153 to 166 ms (12% vs 20%), and QRS >166 (10% vs 24%).
Based on the evidence, patients who are inadequately treated, have serious comorbidities with a life expectancy of <1 year, or are within 40 days post MI and have had HF <3 months should not receive an ICD. Patients without an LBBB who have a QRS <150 ms should not receive CRT.
Impact of Evidence-Based ICD Implantation on Mortality
Michael R. Gold, MD, Medical University of South Carolina, Charleston, South Carolina, USA, reviewed evidence that has demonstrated the benefit of ICDs in eligible patients with HF. The risk of death in patients who were treated with an ICD versus medical therapy was significantly reduced in the Multicenter Unsustained Tachycardia Trial (24% vs 55%; p<0.001) [MUSTT; Buxton AE. N Engl J Med 1999]. In the MADIT-II trial, patients who were treated with an ICD had reductions in the rates of death of 12% at 1 year (nominal 95% CI, −27% to 40%), 28% at 2 years (nominal 95% CI, 4% to 46%), and 28% at 3 years (nominal 95% CI, 5% to 46%; nominal p=0.007) [Moss A et al. N Engl J Med 2002]. The Sudden Cardiac Death in Heart Failure Trial [SCD HeFT; Bardy GH et al. N Engl J Med 2005] enrolled patients with dilated cardiomyopathy with or without coronary artery disease (CAD) and HF (New York Heart Association [NYHA] Class II or III) with LVEF ≤35% and randomly assigned them to ICD, amiodarone, or placebo. Patients in the ICD arm had significantly improved survival (HR, 0.77; 97.5% CI, 0.62 to 0.96; p=0.007) versus those in the placebo arm. Patients with NYHA Class II HF benefitted from ICD therapy (HR, 0.54; 97.5% CI, 0.40 to 0.74; p<0.001); those with NYHA Class III HF did not benefit (HR, 1.16; 97.5% CI, 0.84 to 1.61; p=0.30). Patients with LVEF ≤30% benefitted (HR, 0.73; 97.5% CI, 0.57 to 0.92), but those with LVEF >30% did not (HR, 1.08; 97.5% CI, 0.57 to 2.07).
In the Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure trial [COMPANION; Bristow MR et al. Journal of Cardiac Failure 2000], the risk of death or hospitalization was significantly reduced in patients who received CRT-D versus OMT (RR, 20%; p=0.007) or CRT versus OMT (RR, 20%; p=0.008). All-cause mortality was reduced in patients who received a CRT-D (RR, 36%; p=0.003) but was only marginally reduced in patients who received CRT (RR, 24%; p=0.060). Patients in the MADIT-CRT trial who were treated with CRT-D had improved survival versus patients who received ICD only (p<0.001) [Moss AJ et al. N Engl J Med 2009].
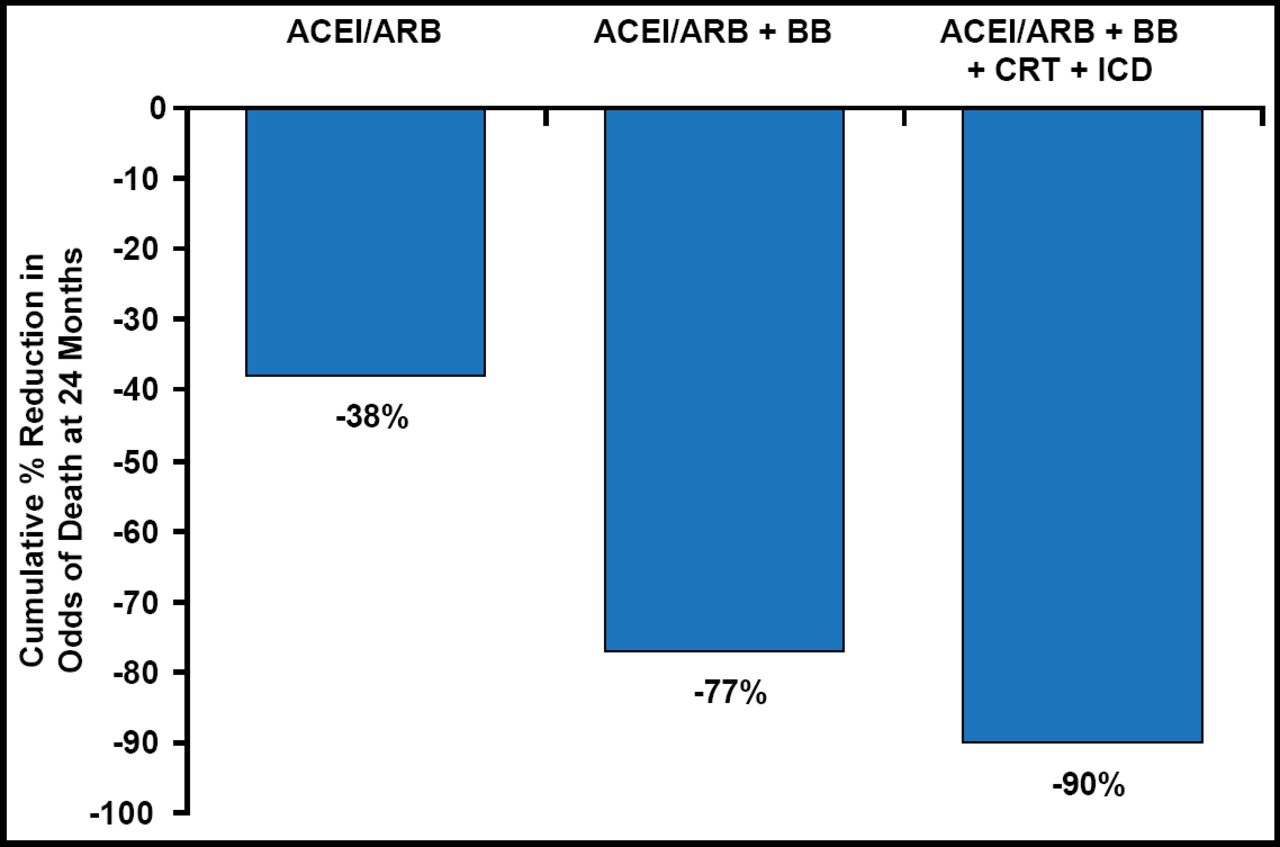
In the Resynchronization/Defibrillation for Ambulatory Heart Failure Trial [RAFT; Tang ASL et al. N Engl J Med 2010], patients who were treated with ICD-CRT versus ICD only had reduced HF death or hospitalization (HR, 0.73; 95% CI, 0.61 to 0.88; p=0.001) and all-cause mortality (HR, 0.71; 95% CI, 0.56 to 0.91; p=0.006). In the REVERSE trial, HF hospitalization or death occurred in 11.7% of patients with CRT turned on versus 24.0% with CRT turned off (HR, 0.38; 95% CI, 0.20 to 0.73; p=0.003). A nested case-control analysis of the Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting [IMPROVE HF] demonstrated greater incremental benefits in the risk of death in patients who were treated with an ICD plus medical therapy [Fonarow GC et al. Am Heart J 2012] (Figure 1). Death rates were reduced by a number of therapies (Table 1).
Death Rate Reduction by Therapy.
Dr. Gold concluded that better utilization of ICDs in indicated HF patients would have a major impact on survival.

Incremental Benefits in the Risk of Death.
ACEI=angiotensin-converting enzyme inhibitor; ARB=angiotensin receptor blocker; BB=beta blocker; CRT=cardiac resynchronization therapy; ICD=implantable cardioverter defibrillator.
Reproduced with permission from MR Gold, MD.
Improving Compliance with ICD Implant Guidelines in HF Patients
Evidence-based therapies, including medical therapy, ICD, and CRT-ICD, have been demonstrated to reduce mortality in patients with HF, but these therapies are underutilized, for example ICDs, and are implanted in only 49% of eligible patients [Fonarow GC et al. Circ Heart Fail 2008]. Clyde W. Yancy, MD, Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA, discussed the benefits of adhering to guidelines as well as methods for improving adherence.
Dr. Yancy's group conducted a clinical practice performance improvement intervention study in HF patients [Fonarow GC et al. Circulation 2010]. Interventions included a 1-day workshop after baseline data were collected, a guideline-based clinical decision tool kit, and Web-based quality-of-care reports. At 24 months, the mean total composite score increased from 68.4% to 80.1% (p<0.001). The percentage of patients who received all indicated quality measures nearly doubled from 24.3% at baseline to 43.9% at 24 months (p<0.001).
Recent results from a study of factors that are associated with improvement in guideline-based use of ICDs demonstrated greater adherence to guideline-recommended use of ICD therapy from baseline to 24 months in cardiology practices that are affiliated with a university or teaching facility compared with outpatient community practices (OR, 2.23; 95% CI, 1.21 to 4.12; p=0.011) and multispecialty practices compared with outpatient community multispecialty practices (OR, 1.76; 95% CI, 1.14 to 2.72; p=0.011) [Mehra MR et al. Pacing Clin Electrophysiol 2012]. An outcomes analysis at 24 months showed significantly lower baseline process conformity for 5 of 7 individual measures among patients who died versus those who survived [Fonarow GC et al. Circulation 2011] (Figure 2).

Process Conformity.
AA=aldosterone antagonist; CRT-D=CRT plus ICD; CRT-P=CRT plus pacemaker; ICD=implantable cardioverter defibrillator.
Reproduced with permission from C. Yancy, MD.
Baseline measure conformity for patients who were alive at 24 months versus those who died, respectively, was:
-
82% versus 72% for patients who received angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB; p<0.001)
-
88% versus 81% for patients who received a β-blocker (p=0.001)
-
35% versus 36% for patients who received an aldosterone antagonist (p=0.56)
-
72% versus 65% for patients who received anticoagulation for atrial fibrillation (AF; p=0.0002)
-
40% versus 34% for patients with CRT plus pacemaker (CRT-P)/CRT-D (p=0.03)
-
52% versus 46% for patients with ICD/CRT-D (p<0.001)
-
61% versus 61% for patients who received HF education (p=0.48)
Conformity with 6 measures was associated with reduced mortality, including ICD/CRT-D (adjusted OR, 0.62; 95% CI, 0.51 to 0.75; p<0.0001). Each 10% improvement in guideline-recommended composite care was associated with a 13% lower odds of 24-month mortality (p<0.0001).
Disparities in ICD use across racial and gender subgroups have been reported, with lower rates among black men (33.4%), white women (29.8%), and black women (28.2%) compared with white men (43.6%) [Hernandez AF. JAMA 2007]. Al-Khatib et al. [Circulation 2012] reported notable improvements in ICD use over time among women and minorities, as well as white men, with the use of a quality-focused approach: black women (adjusted OR, 1.82; 95% CI, 1.28 to 2.58; p=0.0008); white women (adjusted OR, 1.30; 95% CI, 1.06 to 1.59; p=0.01); black men (adjusted OR, 1.54; 95% CI, 1.19 to 1.99; p=0.0009); and white men (adjusted OR, 1.25; 95% CI, 1.06 to 1.48; p=0.007).
Dr. Yancy concluded that adherence to HF guidelines can be improved using a quality-focused, performance improvement-based paradigm. Adherence to the guidelines is associated with improved outcomes. Concerns include appropriate selection of candidates, use of optimal concomitant medical therapies, incidence of lead recalls and extractions, and morbidity/mortality that is associated with shocks.
Improving Compliance with ICD Implantation Guidelines
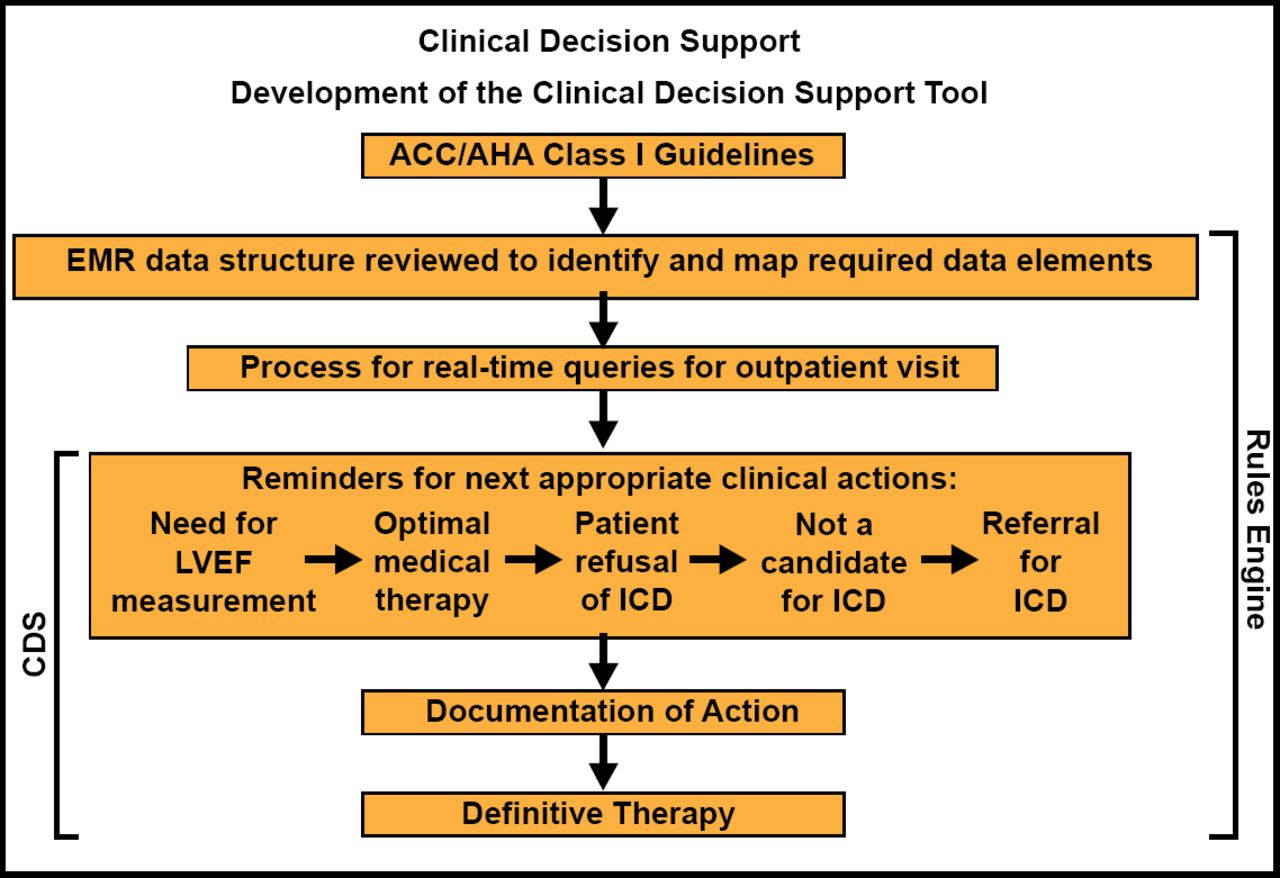
Will Daniel, MD, University of Missouri, Kansas City, Missouri, USA, discussed the use of a clinical decision support (CDS) tool to improve guideline-based therapy use in HF. The CDS tool, which was implemented in 2005, was developed and studied with electronic medical records (EMR+CDS) versus EMR only (Figure 3). The sudden cardiac arrest (SCA) recognition rate was 24% at baseline, 90% in 2006, and 95% in 2007. At 6 months in the SCA recognition process, 41% of patients in the EMR+CDS group versus 11% of those in the EMR group had received an ICD (p<0.001). ICD implantation rates were 18% before the study, 39% in 2006, and 56% in 2007. These results show that improved recognition and use of guideline therapies were sustained for more than 2 years after CDS implementation.

CDS Tool to Support Guideline-Based Therapy.
CDS=clinical decision support; EMR=electronic medical records; LVEF=left ventricular ejection fraction.
Reproduced with permission from W. Daniel, MD.
Rates of ICD implantation were high and similar in men and women (92% vs 95%; p=NS) when the CDS was utilized. However, rates were lower for both sexes, particularly among women, when EMR only was used (men 80% vs women 50%; p<0.0001). Similarly, ICD implantation rates with CDS were similar in men and women (36% vs 33%; p=NS), while ICD implantation rates when only EMR was utilized were lower in both sexes, with a very low rate among women (men 12% vs women 5%; p<0.0001).
CDS improves adherence to guideline-based therapies, makes quality performance measurable and predictable, improves efficiencies for physicians and practices, assists with allocation of physicians' expertise, and can be used for multiple practice disciplines. CDS also eliminates sex and ethnic disparities in ICD implantation.
- © 2012 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.