

Summary
Atrial fibrillation (AF) guidelines recommend identical treatments for stroke prevention for all types of AF (permanent, persistent, paroxysmal), based on known risk factors for stroke. This article discusses the results of a secondary analysis of the Apixaban for the Prevention of Stroke in Subjects with Atrial Fibrillation [ARISTOTLE; NCT00412984] trial, comparing rates of stroke or systemic embolism, bleeding, and mortality by AF type and treatment group.
- Arrhythmias
- Cerebrovascular Disease
- Cerebrovascular Disease Clinical Trials
Atrial fibrillation (AF) guidelines recommend identical treatments for stroke prevention for all types of AF (permanent, persistent, paroxysmal), based on known risk factors for stroke. Several new oral anticoagulants for AF are currently available, including apixaban, a factor Xa inhibitor. Sana M. Al-Khatib, MD, MHS, Duke University, Durham, North Carolina, USA, presented the results of a secondary analysis of the Apixaban for the Prevention of Stroke in Subjects with Atrial Fibrillation [ARISTOTLE; NCT00412984] trial, comparing rates of stroke or systemic embolism, bleeding, and mortality by AF type and treatment group.
Secondary Analysis of ARISTOTLE Trial
In the ARISTOTLE trial [Granger CB et al. N Engl J Med 2011], 18,201 patients with AF and at least 1 additional risk factor for stroke were randomly assigned to treatment with apixaban 5 mg BID or warfarin (target INR 2–3). The primary outcome was stroke or systemic embolism (SE). The primary analysis found a 21% relative risk reduction (RRR) for stroke or SE and a 31% RRR for ISTH major bleeding in patients who were treated with apixaban versus warfarin. The secondary analyses compared outcomes in 2786 patients with paroxysmal AF with 15,412 patients with persistent or permanent AF at study entry.
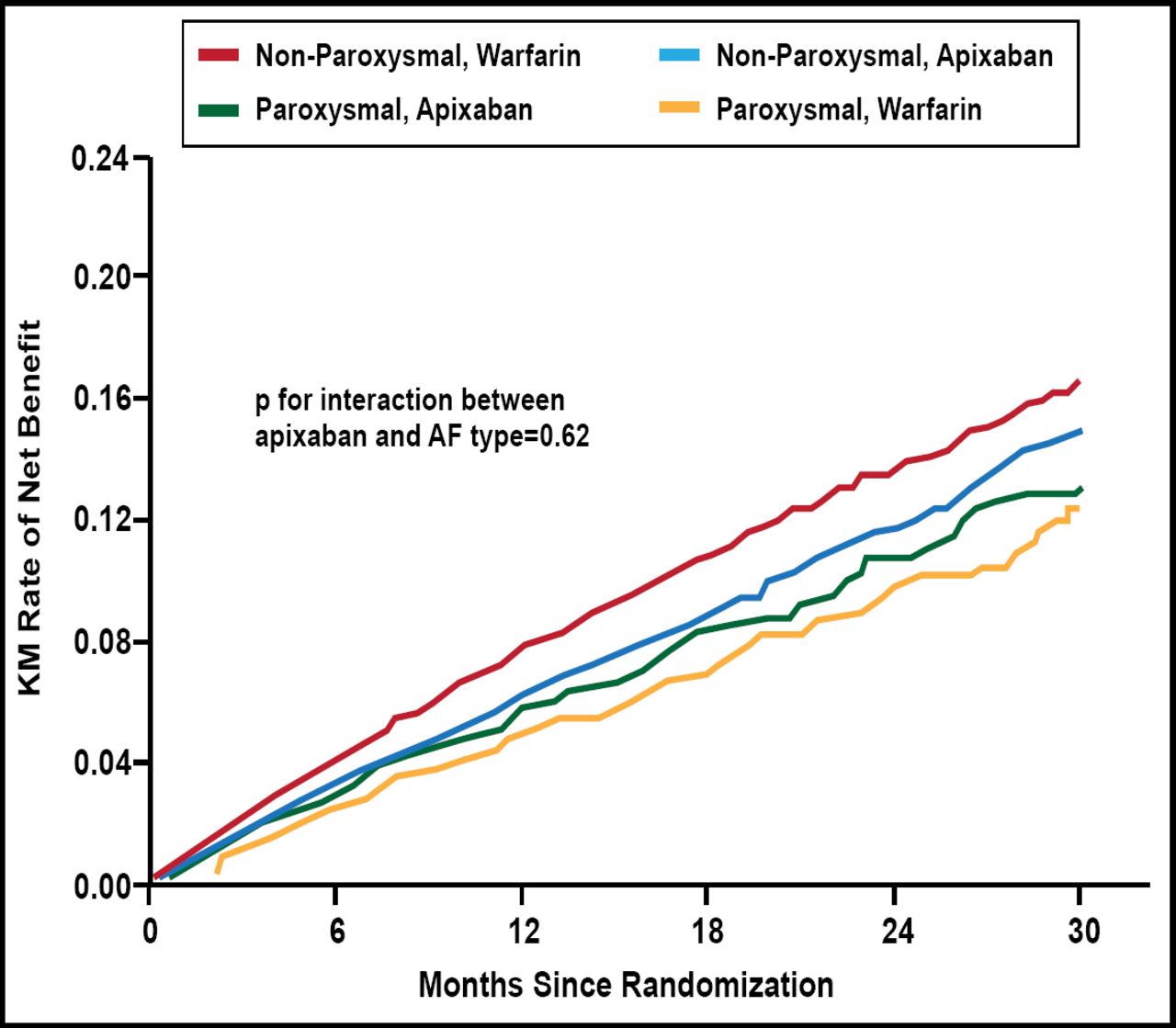
The rate of stroke or SE was significantly lower in patients with paroxysmal AF than in patients with persistent or permanent AF (adjusted HR, 0.70; 95% CI, 0.51 to 0.93; p=0.015). There was no significant difference in the rate of major bleeding among patients with persistent or permanent AF versus those with paroxysmal AF. All-cause mortality tended to be lower in patients with paroxysmal AF versus those with persistent or permanent AF (HR, 0.85; 95% CI, 0.71 to 1.01; p=0.068). There were consistent reductions in stroke or SE (p for interaction=0.71), major bleeding (p for interaction=0.75), and all-cause mortality (p for interaction=0.50) with apixaban in both AF types, as was seen in the overall population (Figure 1). Apixaban provided a more favorable net clinical outcome (stroke or SE, all-cause death, major bleeding) than warfarin in both types of AF (p for interaction between apixaban and AF type=0.62), consistent with the main trial findings (Figure 2).

Outcomes by Type of AF and Study Treatment.
Reproduced with permission from SM Al-Khatib, MD, MHS.

Net Benefit. Stroke or SE, All-Cause Death, Major Bleeding.
Reproduced with permission from SM Al-Khatib, MD, MHS.
In this study, the risk of stroke or SE was higher in patients with persistent or permanent AF than in patients with paroxysmal AF. Compared with warfarin, the effects of apixaban were consistent among patients with paroxysmal AF and those with persistent or permanent AF. Apixaban is an attractive alternative to warfarin in patients with AF and at least 1 other risk factor for stroke or SE, regardless of the type of AF.
- © 2012 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.