

Summary
This article reviews evidence from the past 20 years on the benefits and risks of antiplatelet therapy for primary and secondary prevention of vascular events.
- Thrombotic Disorders
Louise Bowman, MBBS, MRCP, University of Oxford, Oxford, United Kingdom, reviewed evidence from the past 20 years on the benefits and risks of antiplatelet therapy for primary and secondary prevention of vascular events. The landmark ISIS-2 trial [ISIS-2 Collaborative Group. Lancet 1988] compared vascular mortality rates in patients after suspected acute myocardial infarction. Investigators reported vascular mortality rates of 13% in patients who received routine hospital care alone, 11% in those treated with aspirin only, 10% in those treated with streptokinase only, and 8% in those who received routine care plus aspirin and streptokinase.
An analysis of 25 secondary prevention trials (25,000 patients) found that antiplatelet therapy reduced the incidence of serious vascular events by about 25% among patients at risk for occlusive vascular disease [Antiplatelet Trialists' Collaboration. Br Med J (Clin Res Ed) 1988]. However, researchers noted that the balance of risks and benefits might be different for primary prevention in low-risk individuals. A 1994 meta-analysis [Antiplatelet Trialists' (ATT) Collaboration. BMJ 1994] of 145 trials of 70,000 high-risk and 30,000 low-risk subjects receiving antiplatelet therapy versus control and 10,000 high-risk subjects receiving different antiplatelet regimens found a significant benefit from antiplatelet therapy. The study provided no clear evidence on the balance of risks and benefits for primary prevention in low-risk subjects.
The ATT Collaboration evaluated the effects of antiplatelet therapy on vascular events in 212,000 high-risk patients from 287 trials [BMJ 2002]. The investigators found a significant odds reduction in most subgroups of individuals treated with antiplatelet therapy versus control, except diabetes patients, in whom the benefit was not clear. Despite this uncertainty, most guidelines recommend antiplatelet therapy for diabetes patients.
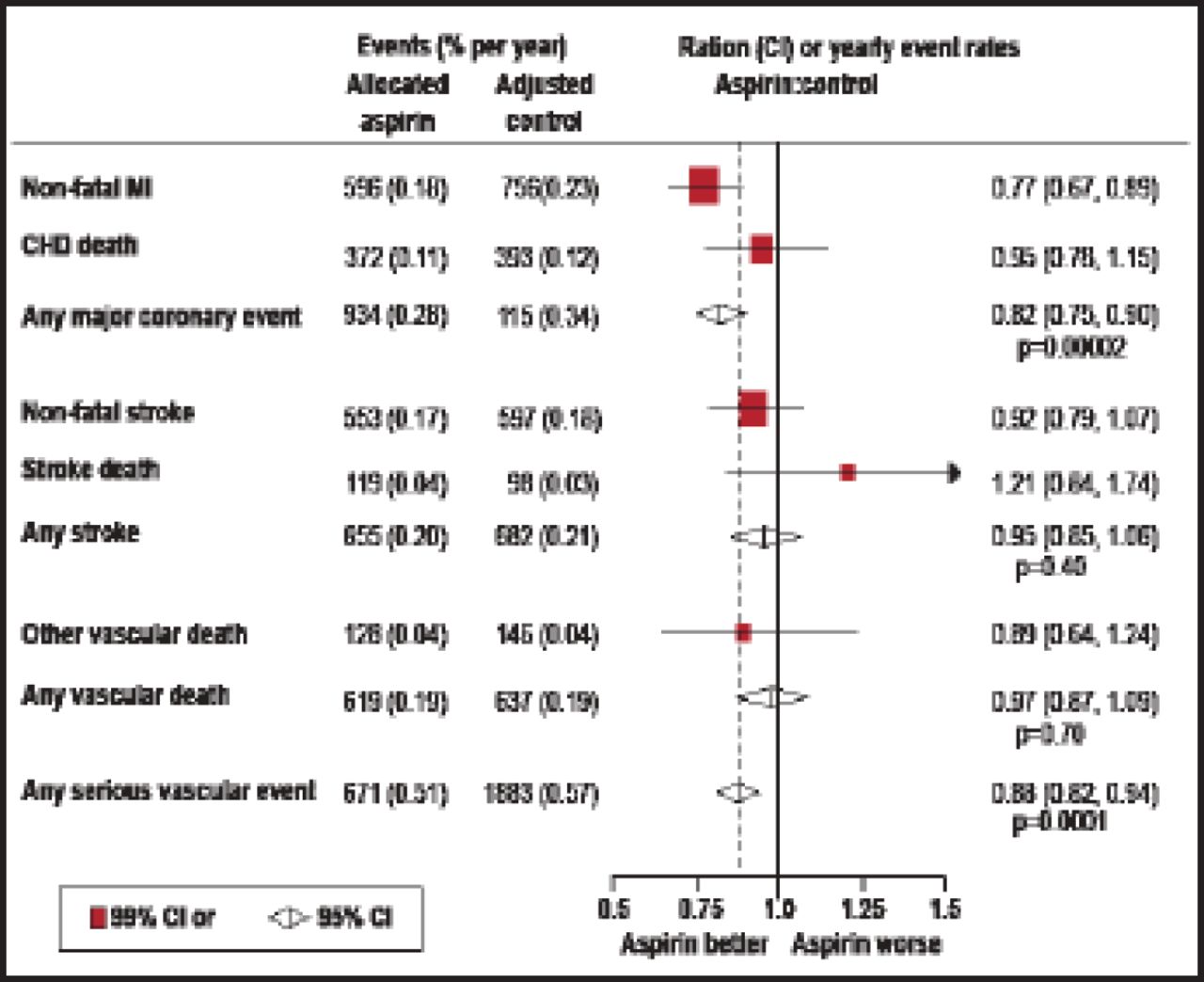
The absolute risk of bleeding with aspirin is increased in the elderly, men, diabetes patients, and smokers. Aspirin is associated with a 30% increased risk of intracranial bleeding and a 50% increase in extracranial bleeding. The ATT Collaboration analyzed 6 primary prevention trials of aspirin versus control involving 95,456 patients [Lancet 2009]. The meta-analysis showed that aspirin reduced the odds for major coronary events and any serious vascular event but showed no clear benefit in stroke reduction (Figure 1). Patients at higher risk of vascular events (the elderly, men, diabetes patients, and smokers) also had a 1.6- to 2.2-fold higher risk of bleeding with aspirin. Several ongoing clinical trials are evaluating aspirin therapy in patients with diabetes, cardiovascular disease risk, and the elderly.

Proportional Effects of Aspirin on Serious Vascular Events in Primary Prevention Trials.
CHD=coronary heart disease; MI=myocardial infarction.
Reproduced with permission from Elsevier. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Antithrombotic Trialists' Collaboration. The Lancet 2009;373(9678): 1849–1860.
Dr. Bowman concluded that the benefits of using antiplatelet therapy for secondary prevention outweigh the risks. Questions remain about the suitability of antiplatelet therapy for primary prevention. Ongoing trials will help to answer some of these questions in the next few years.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.