

Summary
Coronary computed tomographic angiography (CCTA) is an emerging tool for the noninvasive assessment of coronary artery disease (CAD) [Arbab-Zadeh A et al. J Am Coll Cardiol 2012]. Although coronary angiography (CA) is the gold standard for diagnosing CAD, it is an invasive and expensive procedure with a small (0.1% to 0.2%) risk of major complications, such as death, myocardial infarction, and stroke [Mowatt G et al. Health Technol Assess 2008]. This article discusses a study on the correlations between outcomes from 64-slice CCTA with retrospective gating and CA.
- Imaging Modalities
- Coronary Artery Disease
- Radiography
- Interventional Radiology
- Cardiac Imaging Techniques
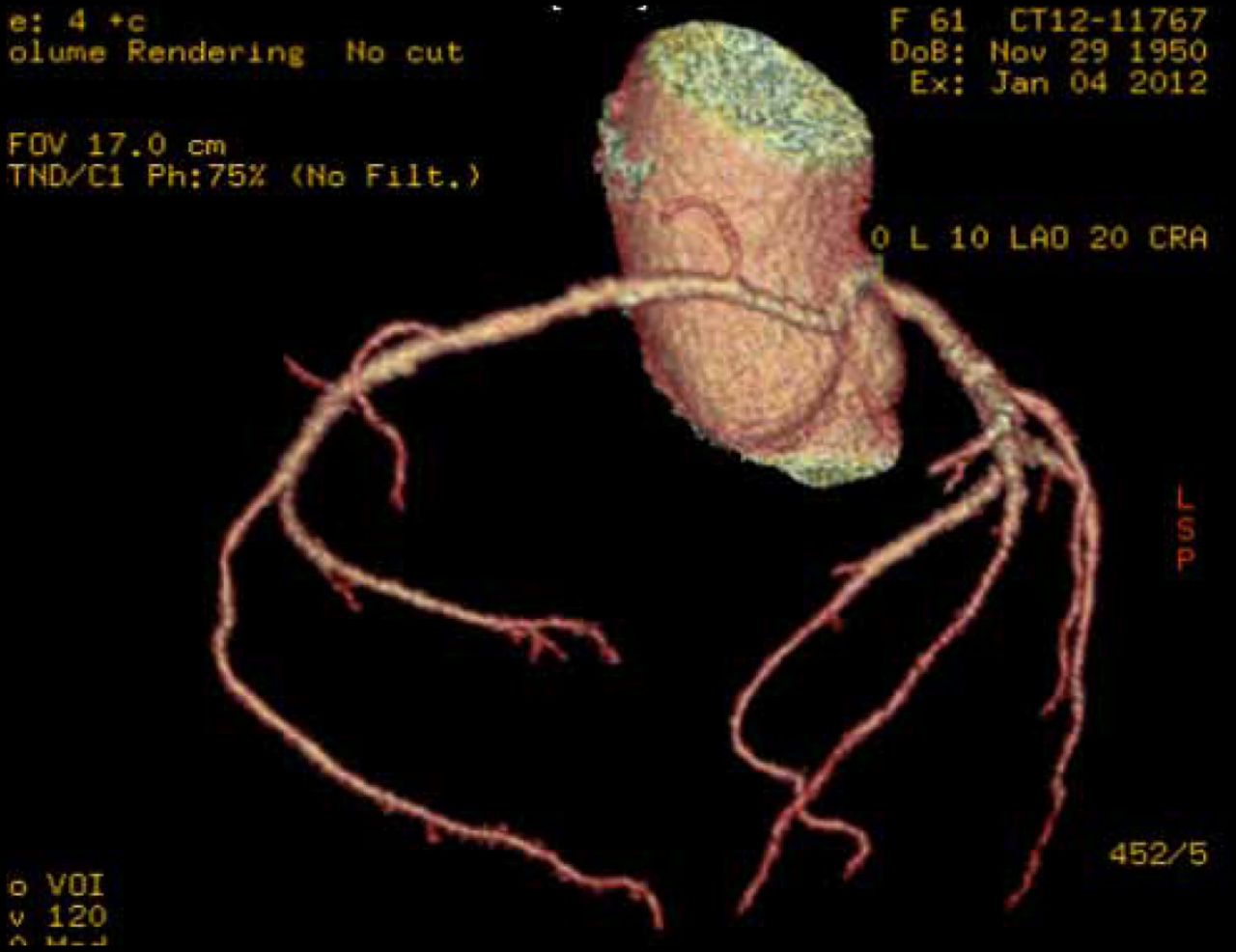
Coronary computed tomographic angiography (CCTA) is an emerging tool for the noninvasive assessment of coronary artery disease (CAD) [Arbab-Zadeh A et al. J Am Coll Cardiol 2012]. Although coronary angiography (CA) is the gold standard for diagnosing CAD, it is an invasive and expensive procedure with a small (0.1% to 0.2%) risk of major complications, such as death, myocardial infarction, and stroke [Mowatt G et al. Health Technol Assess 2008]. Raymond Massay, MD, Bracebridge Medical Center, St. Michael, Barbados, discussed a study on the correlations between outcomes from 64-slice CCTA with retrospective gating and CA (Figure 1 and 2).

Left Anterior Descending Artery Angle: −44.0.
Reproduced with permission from R. Massay, MD.

Volume Rendering; No Cut.
Reproduced with permission from R. Massay, MD.
The study staff at Dr. Massay's center includes 2 cardiologists, 2 radiologists, a visiting cardiac radiologist, and 2 CT radiographers. Eligible patients for CCTA included those who were asymptomatic with abnormal baseline electrocardiograms (ECGs; ie, complete left bundle branch block, T-wave changes, and marked ST) that made it difficult to interpret stress ECGs, symptomatic patients unable to do a treadmill stress test. and those with an equivocal treadmill stress test (ie, symptomatically negative but electrically positive or symptomatically positive but electrically negative).
Minor indications included a high Framingham Risk Score; dilated cardiomyopathy. recurrence of clinical symptoms in a population with metabolic syndrome. or patients >50 years of age with coronary heart or valve disease needing heart surgery/intervention. Patients with active arrhythmias were excluded from the study.
To achieve the low and regular heart rate necessary for optimal imaging (ie, <70 beats per minute [bpm]), patients were administered atenolol 100 mg daily × 5 days, nadolol 80 mg daily × 5 days, bisoprolol 5 mg daily × 5 days, and/or metoprolol 5 to 10 mg intravenously (IV) if still needed to bring the heart rate to <70 bpm. Sublingual glyceryl trinitrate was used for coronary dilation. Patients avoided stimulants and ate a light breakfast.
Enrollment began in February 2010 and ended in May 2012. The sample included a total of 211 patients (57% male). The median age was 55 years, with a range from 34 to 85 years. Complications included 1 case of acute bronchospasm, an allergic reaction in 1 patient, incomplete tests in 2 patients; an inability to get good IV access in 1 patient, and claustrophobia in 1 patient. A total of 16 patients had CA. The association with CCTA was positive in 12 cases and negative in 4. Among those who had CA, 6 patients had percutaneous coronary intervention and 2 had coronary artery bypass graft surgery.
According to Dr. Massay, CCTA service in Barbados is now well established and safe, with an acceptable degree of accuracy. Future plans for the use of the technology call for myocardial tissue characterization and identification of valve disease. CCTA will also serve as an adjunct to intervention for assessment of fractional flow reserve and see increased use in the management of chest pain in the acute setting.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.