

Summary
Teratomas are benign germ-cell tumors that occur in infants through young adults. They contain cell types from at least 2 of 3 primitive germ cell layers. Ectodermal elements often predominate (hair, skin, sweat gland, or tooth-like structures), as well as mesodermal (fat, cartilage, smooth muscle, bone) or endodermal (respiratory and intestinal epithelium) elements. Pericardial teratomas most commonly arise in the anterior superior mediastinum. These tumors usually are diagnosed in infants and children <10 months of age at a rate of 5 to 6 per 10,000 children. They are exceptionally rare in adults.
- Interventional Techniques & Devices Imaging Modalities
Teratomas are benign germ-cell tumors that occur in infants through young adults. They contain cell types from at least 2 of 3 primitive germ cell layers. Ectodermal elements often predominate (hair, skin, sweat gland, or tooth-like structures), as well as mesodermal (fat, cartilage, smooth muscle, bone) or endodermal (respiratory and intestinal epithelium) elements. Pericardial teratomas most commonly arise in the anterior superior mediastinum. These tumors usually are diagnosed in infants and children <10 months of age at a rate of 5 to 6 per 10,000 children. They are exceptionally rare in adults.
Pericardial teratomas may be asymptomatic or cause chest pain, cough, dyspnea, and/or cardiac tamponade. In infants they present with respiratory distress and/or hydrops fetalis. They usually present as right-sided masses near the aortic root, superior vena cava, right atrium, and pulmonary artery (Figure 1). In rare cases, mature teratomas undergo malignant transformation. Chest radiography often demonstrates an enlarged mediastinum or cardiac silhouette. Computerized tomography (CT) demonstrates a well-circumscribed anterior mediastinal mass which is usually heterogenous in composition. Magnetic resonance imaging (MRI) confirms pericardial involvement and often reveals a large mass of heterogenous fluid intensity. The outcome for benign pericardial teratomas is favorable with complete surgical resection. Incomplete resection can result in residual pericardial effusion and tamponade.

Pericardial Teratoma.
Reproduced with permission from S. Lalla, MBBS.
Sasha Lalla, MBBS Advanced Cardiovascular Institute, Port of Spain, Trinidad and Tobago, described the case of a 42-year-old Afro-Caribbean woman presenting with atypical chest pain and NYHA Class II dyspnea. She had a history of essential hypertension, diabetes, and sickle cell trait. There was no history of coronary artery disease; she was a nonsmoker, and used little alcohol. The physical examination and vital signs were normal.
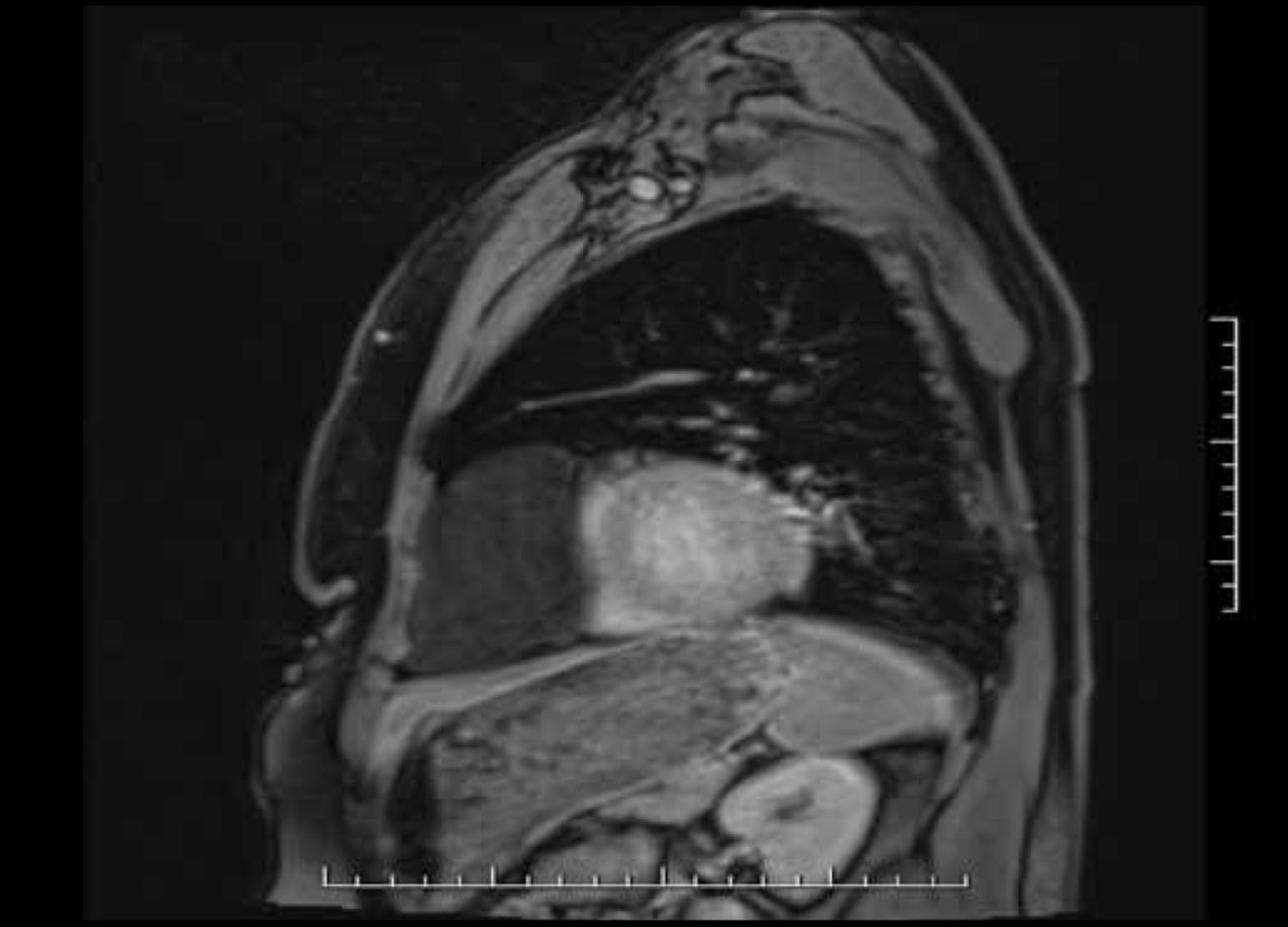
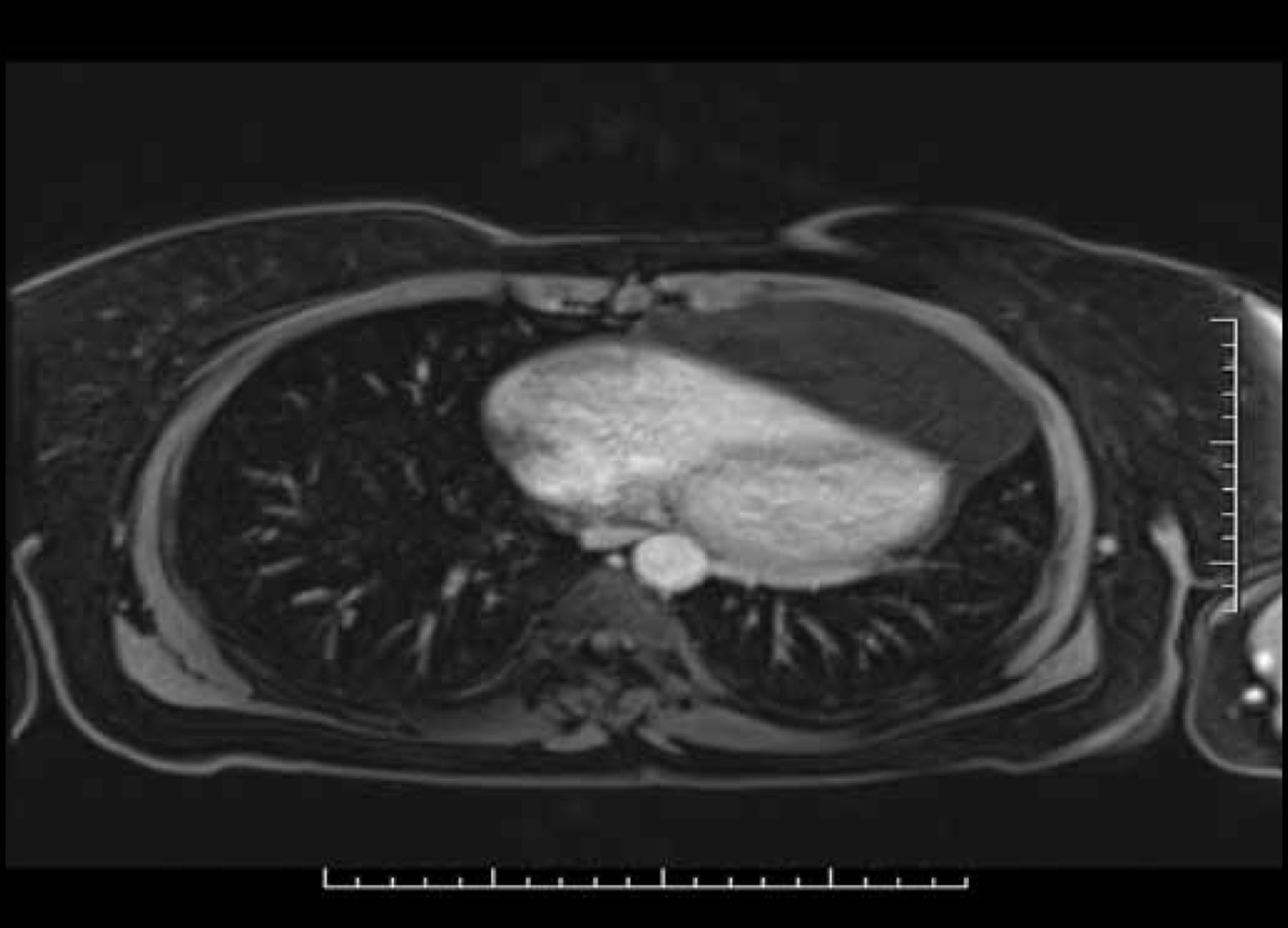
The electrocardiogram showed normal sinus rhythm with normal intervals, low voltage QRS, incomplete right bundle branch block, and nonspecific T-wave abnormality. CT showed a large well-defined thin-walled cystic mass in the anterior inferior mediastinum anterior to the ventricles, with posterior displacement of the heart within the left hemithorax (Figures 2 and 3). The mass measured 20 cm from the origin of the pulmonary outflow tract to the lung base. Echocardiogram showed a prominent extrapericardial echolucent area anterior to the right ventricle (RV) with off-axis heart position but no significant RV compression. MRI showed RV free wall distortion and restriction to RV diastolic expansion. The mass was homogeneous with no invasion of the RV and no pericardial thickening. Coronary angiogram revealed normal coronary arteries.

Cystic Mass.
Reproduced with permission from S. Lalla, MBBS.

Cystic Mass.
Reproduced with permission from S. Lalla, MBBS.
A surgical decision was made to excise the mass due to its compressive nature and the symptoms produced. This was achieved via median sternotomy without arrest of the heart. The mass was excised intact and the pericardium left intact. The mass was an enlarged pericardial cyst (12.6 cm diameter) extending into the left costophrenic angle, grossly described as a cystic mass 10 × 8 × 1.5 cm. The cyst was multilobulated with septations and thin-walled with a smooth lining containing clear fluid and fatty tissue. At the point of surgery the tentative diagnosis was that of a pericardial cyst but definitive histology revealed a cyst lined with a single layer of cuboidal cells, containing tiny bone spicule and hair fragments, suggestive of a benign cystic pericardial teratoma. The patient had an uneventful postoperative course and was asymptomatic at follow-up.
This case describes a pericardial teratoma presenting as a noncoronary cause of chest pain and effort intolerance and masquerading as a benign pericardial cyst. It illustrates the fact that multimodal imaging of cardiac neoplasms—though useful in delineating anatomy and the relation of masses to surrounding structures—may only provide limited information. A true and accurate diagnosis often cannot be established until definitive pathologic assessment following surgical biopsy underscoring its importance, as in this case.
The work of Drs. Randolph Rawlins, Ronald Henry, Taarik Dookie, Eamon Foster, and Sasha Lalla and the Advanced Cardiac Institute Surgical Therapies, Trinidad and Tobago, are acknowledged for their collaboration on this case.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.