

Summary
Atrial fibrillation (AF) in patients with heart failure (HF) is a growing problem because of the increasing incidence of HF related to long-standing hypertension, atrial remodeling due to elevated left ventricular diastolic pressure in HF patients, and the increasing age of the population. This article discusses the treatment of AF in HF patients.
- Arrhythmias
- Heart Failure
Atrial fibrillation (AF) in patients with heart failure (HF) is a growing problem because of the increasing incidence of HF related to long-standing hypertension, atrial remodeling due to elevated left ventricular diastolic pressure (LVEDP) in HF patients, and the increasing age of the population. Alfred A. Bove, MD, PhD, Temple University Medical School, Philadelphia, Pennsylvania, USA, discussed the treatment of AF in HF patients.
The severity of HF and the incidence of AF are positively correlated; about half of patients with NYHA Class IV HF develop AF [Savelieva I and Camm AJ. Europace 2004]. Ten-year outcomes from the Framingham study showed that 35% of patients with HF developed AF and 28% of patients with AF developed HF [Wang TJ et al. Circulation 2003]. The Euro Heart Failure study included 10,701 patients hospitalized with HF; 3673 had previous AF, 1001 had new AF, and 6027 did not have AF [Rivero-Ayerza M et al. Eur Heart J 2008]. Patients with new-onset AF spent the most days in the intensive care unit (ICU), while those with previous or no AF had the same number of ICU days. Patients with AF when admitted had a mortality rate of 7% compared with about 13% in patients with new AF.
In the Get with the Guidelines Registry (US), 31.4% of 99,810 patients admitted for HF had AF [Mountantonakis SE et al. Circ Heart Fail 2012]. Approximately 41.5% of patients in normal sinus rhythm were hospitalized >4 days compared with 48.8% of those with AF. Hospital mortality was higher in patients with AF (4.0%) than in those without AF (2.6%).
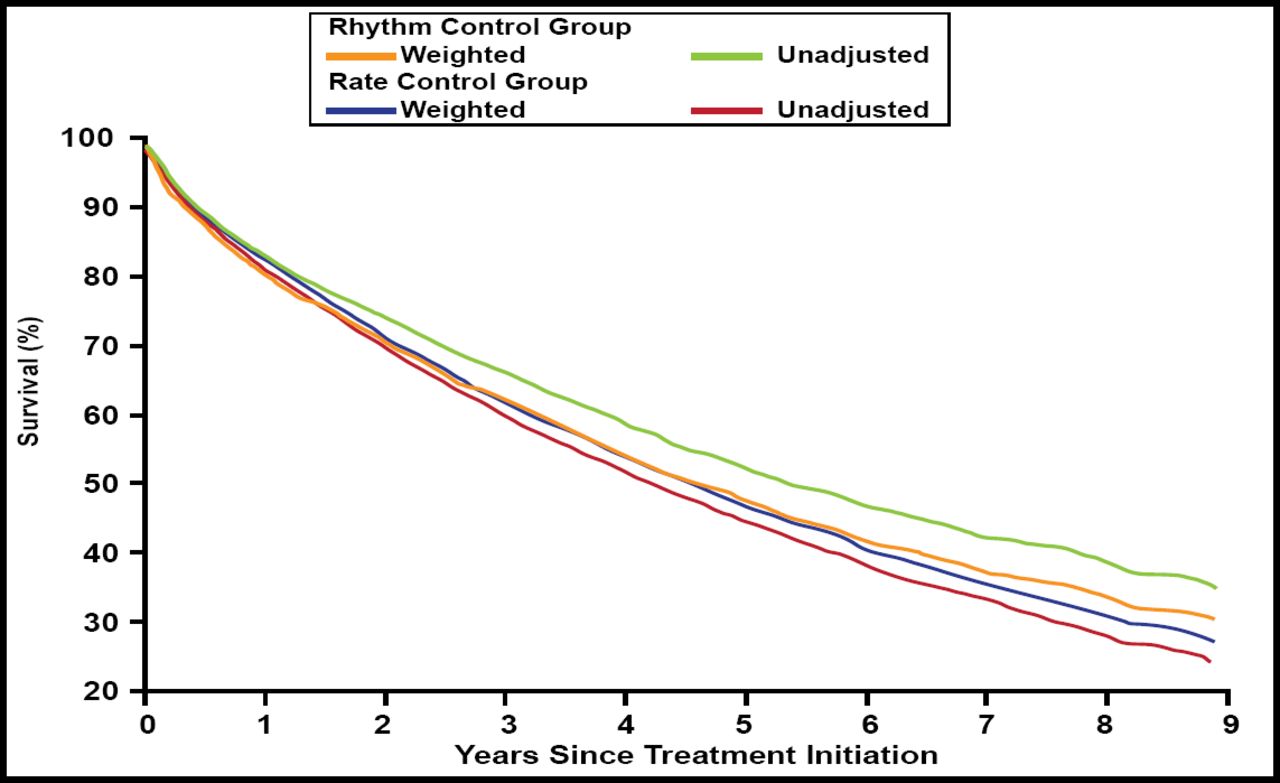
A study of 1376 patients with NYHA class III/IV HF and AF evaluated rhythm control (n=682) versus rate control (n=694) for AF [Roy D et al. N Engl J Med 2008]. The Kaplan-Meier curves showed no significant difference between the 2 groups for worsening HF, stroke, and death from any cause. In the Atrial Fibrillation Follow-Up Investigation of Rhythm Management [AFFIRM] trial of rhythm versus rate control for AF, 1 to 3 year outcomes were the same for the rhythm and rate control groups [Ionescu-Ittu R et al. Arch Intern Med 2012]. However, mortality significantly decreased in the rhythm control versus rate control group after 5 years (5-year HR, 0.89; 95% CI, 0.81 to 0.96; 8-year HR, 0.77; 95% CI, 0.62 to 0.95; Figure 1).

AFFIRM Rate vs Rhythm Control: Mortality.
AFFIRM=Atrial Fibrillation Follow-up Investigation of Rhythm Management.
Reproduced with permission from F. Bove, MD.
A study of patients with HF and AF treated with rhythm (n=13) versus rate (n=13) control found that LV fractional shortening significantly increased from 20% to 31% with rhythm control (p<0.0001) [Azpitarte J et al. Chest 2001]. Rhythm control patients had significant decreases from baseline in LV end diastolic (LVED) dimension (p=0.014), left atrial diameter (LAD; p=0.003), and heart rate (p<0.0001). These parameters did not change significantly in the rate control group. Lutomsky et al. [Europace 2008] reported that ablation for paroxysmal AF in patients with ejection fraction (EF) <50% resulted in 50% recurrence rate of AF at 5 months and an increase in LVEF from 41%±6% to 51%±12%. Meanwhile, patients with an LVEF ≥50% had a rate of recurrence of AF of only 27% at 5 months. These data justify efforts to maintain or restore sinus rhythm in patients with heart failure.
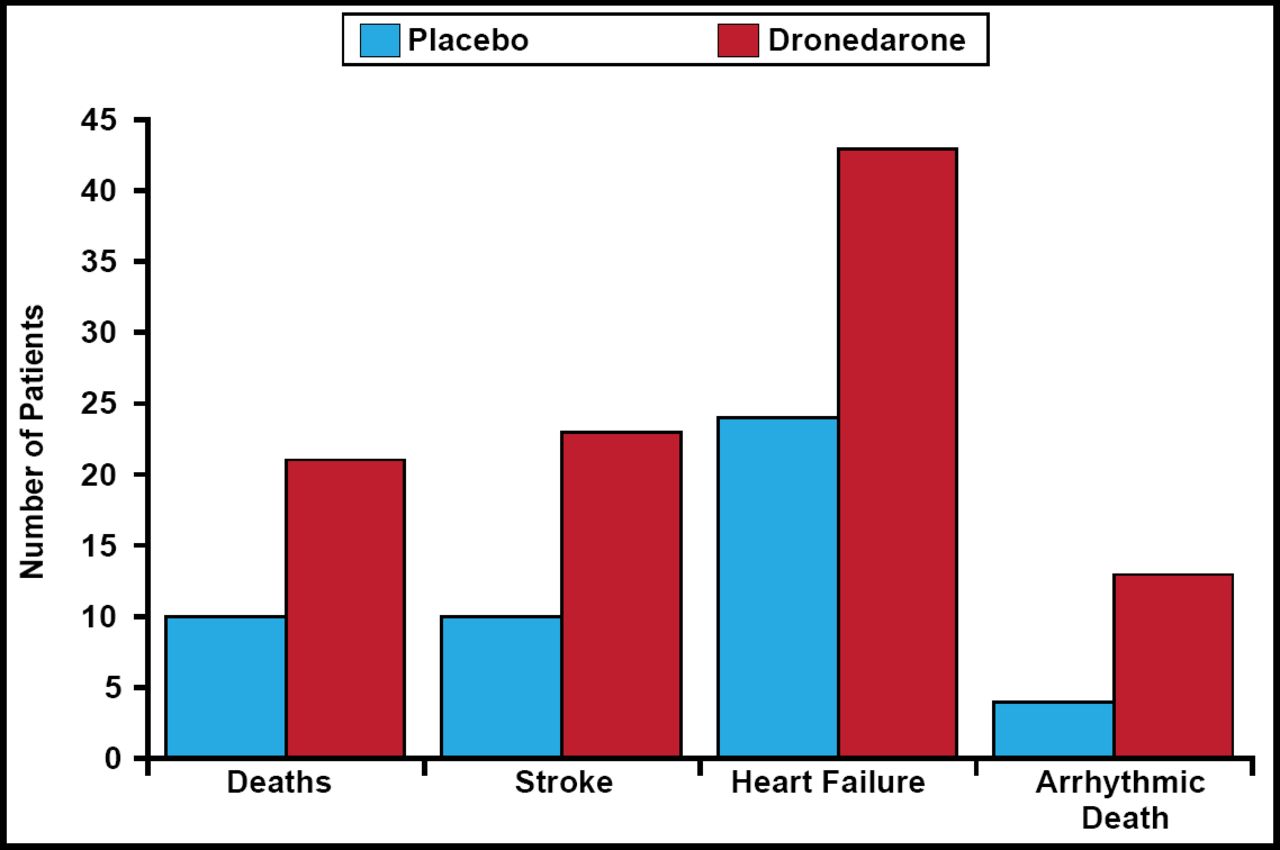
A study of dronedarone in patients with high-risk permanent AF found that dronedarone increased the numbers of patients with HF (43 vs 24; HR, 1.81; 95% CI, 1.10 to 2.99; p=0.02), stroke (23 vs 10; HR, 2.32; 95% CI, 1.11 to 4.88; p=0.02), arrhythmic death (13 vs 4; HR, 3.26; 95% CI, 1.06 to 10.00; p=0.03), and cardiovascular death (21 vs 10; HR, 2.11; 95% CI, 1.00 to 4.49; p=0.046; Figure 2) compared with placebo [Connolly SJ et al. N Engl J Med 2011]. Therefore, dronedarone should be avoided in patients with HF and permanent AF.

Dronedarone Increased Deaths, Stroke, and HF.
HF=heart failure.
Reproduced with permission from F. Bove, MD.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.