

Summary
This article describes the features of computed tomography angiography (CTA) and how these features allow high temporal and spatial resolution of specific cardiac structures. In CTA, the X-ray tube rotates around the patient 3 times per second—much faster than the 1- to 3-second rotation time of conventional CT—providing high temporal resolution. The small size allows creation of high-resolution, artifact-free coronary artery and cardiac reconstructions.
- Tomography
- Cardiac Imaging Techniques
- Radiography
- Coronary Artery Disease
- Imaging Modalities
- Interventional Radiology
High Resolution with CT Angiography
Lawrence M. Boxt, MD, Albany Medical Center, Albany, New York, USA, described the features of computed tomography angiography (CTA) and how these features allow high temporal and spatial resolution of specific cardiac structures. In CTA, the X-ray tube rotates around the patient 3 times per second—much faster than the 1- to 3-second rotation time of conventional CT—providing high temporal resolution. Spatial resolution is high due to the small size (0.6 mm) of the cardiac CT scanner detectors, which ultimately produce 3D images composed of cubes called voxels that are 0.6 mm on a side. The small size allows creation of high-resolution, artifact-free coronary artery and cardiac reconstructions.
CTA data are collected throughout the cardiac cycle, producing a stack of 3D data for each of a series of phases of the cardiac cycle, starting from end diastole through to end systole and back to end diastole. Looking at the data over time allows visualization of cardiac structure as well as cardiac motion. The 3D dataset can be manipulated to select, extract, and view any plane through the heart. Using surface-rendered 3D, part of a structure with a specific attenuation can be identified and the rest of the structure subtracted to produce detailed images of the heart's outer surface. This technique is used for evaluation of coronary artery bypass grafts. Multiplanar reconstruction involves identifying a specific structure such as a coronary artery and locating in each slice to construct multiplanar reconstructions of the entire artery length.
Risks and Benefits of CTA
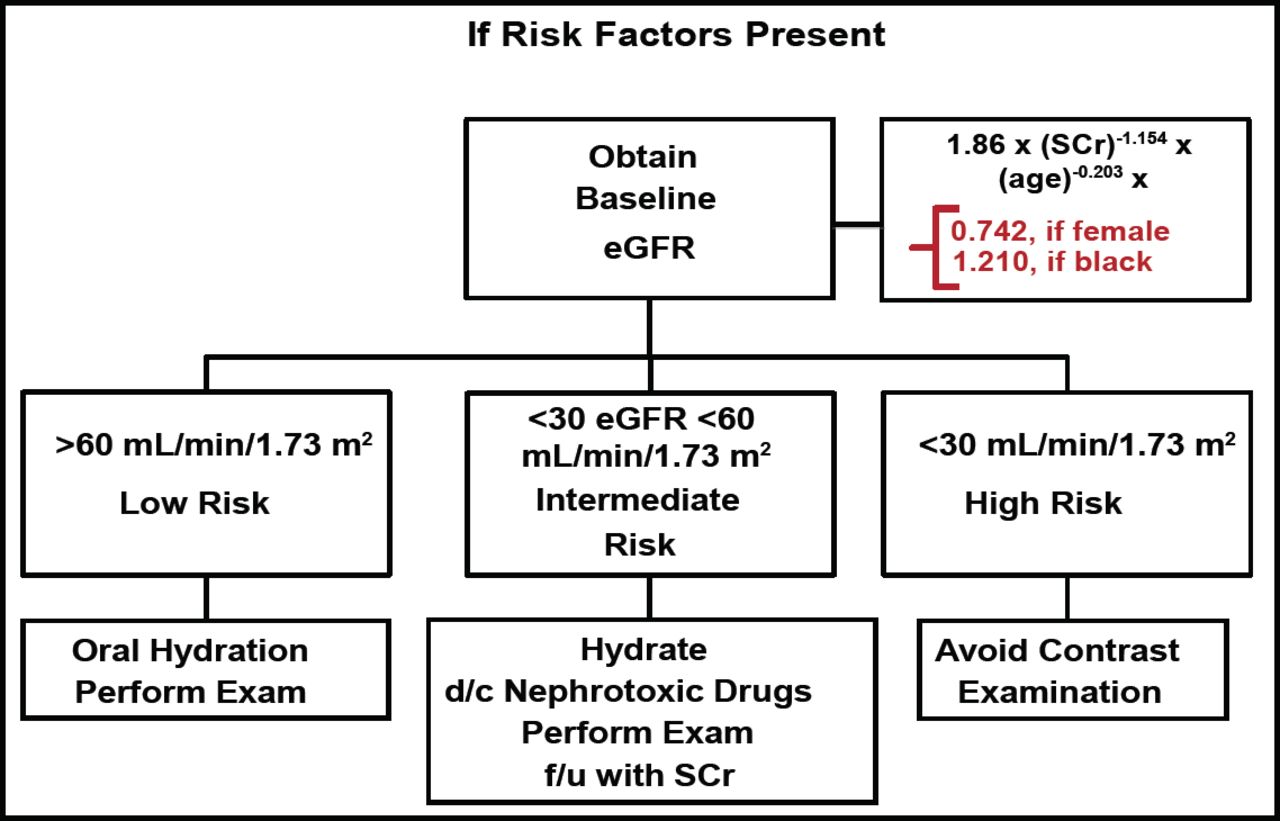
Iodinated contrast media may induce contrast-induced nephropathy (CIN), defined as a 25% increase in serum creatinine (SCr) from baseline, and may result in acute kidney failure. CIN occurs in 3.3% to 8% of contrast administrations in individuals without pre-existing renal impairment and in 12% to 26% of administrations in those with renal disease or diabetes. Patients at risk for CIN can be identified and prevention strategies implemented (Figure 1) [Levey AS et al. Ann Intern Med 2003]. Low-risk patients are given oral hydration prior to CTA.

Evaluation of High CIN Risk and Prevention Strategies.
eGFR=estimated glomerular filtration rate; SCr=serum creatinine.
Reproduced with permission from LM Boxt, MD.
Intermediate-risk patients should receive hydration, discontinue potentially nephrotoxic drugs before CTA, and have follow-up SCr afterwards. Contrast examination should generally be avoided in high-risk patients.
Radiation exposure is another concern. Hausleiter et al. [Circulation 2006] studied the radiation doses received during 16- and 64-slice CTA and the impact of different scan protocols on dose. They found that the higher spatial and temporal resolution of 64-slice CTA is associated with an increased radiation dose compared to 16-slice CTA (14.8±1.8 vs 10.6±1.2 mSv). Dose-modulating algorithms significantly reduced the radiation exposure (Table 1). Dose can also be reduced using the step-and-shoot acquisition technique, which delivers a dose of 2.5±0.8 mSv (range 1.2 to 4.4). Using this technique for diagnosis of significant coronary stenoses, Scheffel et al [Heart 2008] found that the overall patient-based sensitivity, specificity, positive predictive value, and negative predictive value were 100%, 93%, 94%, and 100%, respectively.
16- and 64-Slice CTA Radiation Doses in Patients Scanned with Different Scanning Protocols.
Based on these data and other studies evaluating the accuracy and prognostic value of CTA, Dr. Boxt concluded that CTA is a rapid, safe, and efficient means of investigating patient complaints of chest pain. CTA is a highly sensitive indicator of the absence of coronary artery disease (CAD) and provides morphologic information for CAD risk assessment and clinical prognosis. The risks associated with CTA—namely CIN and radiation exposure—should be considered when determining which imaging procedure is best for a given patient.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.