

Summary
An estimated 26 million American adults have chronic kidney disease (CKD) and millions of others are at increased risk for CKD [National Kidney Foundation]. Furthermore, as glomerular filtration rate falls, the risk of cardiovascular death increases [Go AS et al. N Engl J Med 2004].
- Hypertension & Kidney Disease
- Lipid Disorders
- Hypertensive Disease
- Prevention & Screening
- Renal Disease
An estimated 26 million American adults have chronic kidney disease (CKD) and millions of others are at increased risk for CKD [National Kidney Foundation. www.kidney.org]. Furthermore, as glomerular filtration rate falls, the risk of cardiovascular (CV) death increases [Go AS et al. N Engl J Med 2004].
Robert P. Giugliano, MD, SM, Harvard Medical School, Boston, Massachusetts, USA, reviewed the overlap of CKD and CV risk, highlighted results of key clinical trials and guideline recommendations in patients with CKD and CV disease (CVD), and discussed potential future therapies in this group of patients.
According to Dr. Giugliano, the strong association between CKD and CVD is underappreciated. Patients with CKD have a higher prevalence of both traditional CVD risk factors (eg, hypertension, type 2 diabetes, and dyslipidemia) as well as nontraditional ones, (eg, inflammation, malnutrition, mineral disorders, and anemia). “All patients with CKD, even those with mild-to-moderate renal dysfunction, should be considered at high risk for CV death,” he said, noting an inverse exponential relationship between the 2 diseases.
An overlap of 3 common diseases—diabetes mellitus, hyperlipidemia, and CKD–can help explain why these patients are at hightened risk and point towards common solutions (Figure 1). In 2011, 366 million people worldwide had diabetes; 183 million (50%) were undiagnosed [IDF Diabetes Atlas. The Global Burden www.idf.org]. Patients with type 2 diabetes make up the largest and fastest growing single disease group requiring renal replacement therapy [Vora JP et al. J Hum Hypertens 2000]. The Hypertension Detection and Follow-up Program [Shulman NB et al. Hypertension 1989] found that in CKD patients with creatinine >1.7 mg/dL, 58% died from CVD and 19% from renal failure. General treatment principles at that time included the evaluation and aggressive treatment of CVD risk factors and the assessment of CKD-related factors (eg, proteinuria, anemia, and volume status).
The lipid profile typically seen in renal disease is characterized by high circulating triglycerides, very low-density lipoprotein cholesterol, intermediate-density lipoprotein, cholesterol, chylomicron remnants, low plasma high-density lipoprotein cholesterol particles, and increased levels of lipoprotein A. Numerous studies have shown that lipid derangement is likely to be an independent risk factor for the development of renal disease [Gyebi L et al. Curr Hypertens Rep 2012].
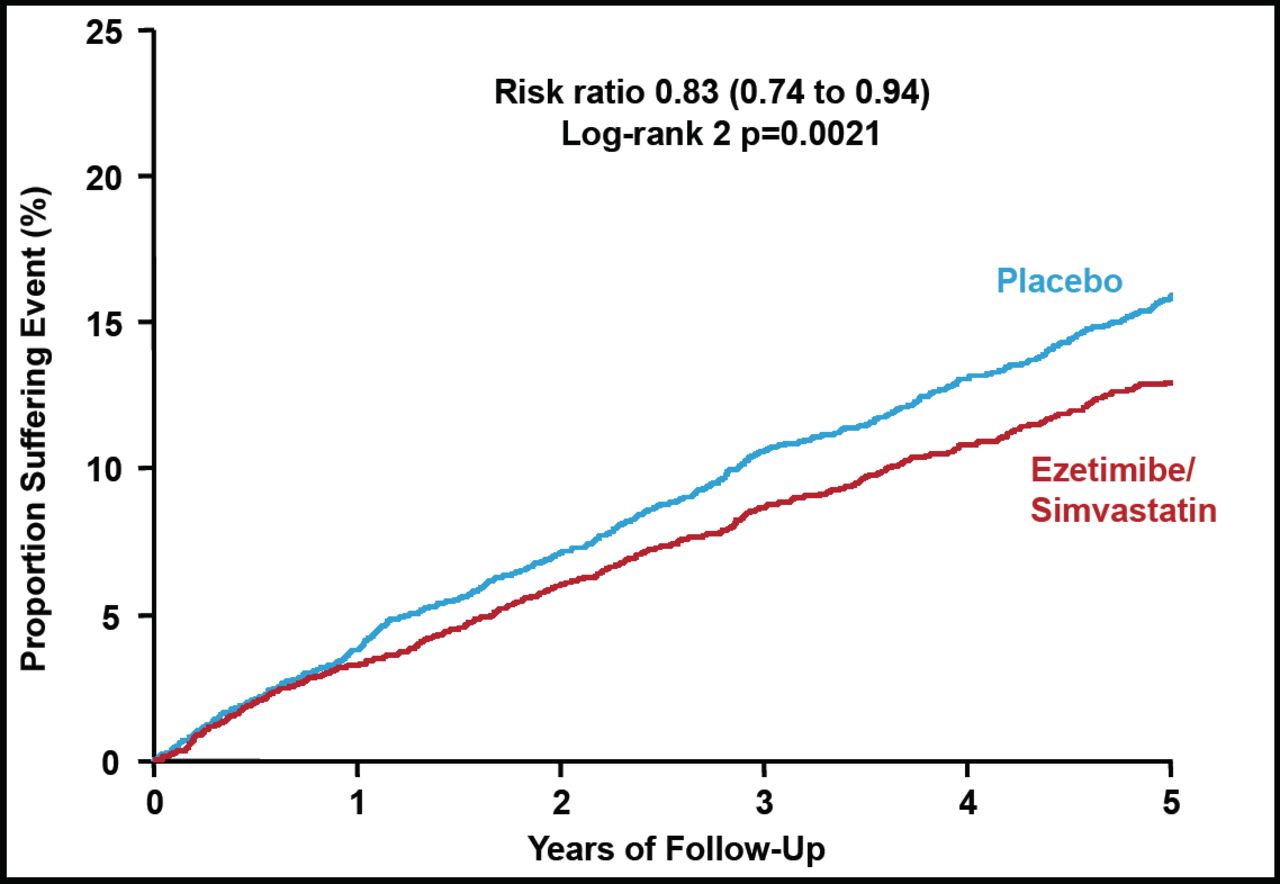
Statin administration in CKD is now common practice endorsed by the Kidney Disease Outcomes Quality Initiative (KDOQI) [Ruan XZ et al. Nat Rev Nephrol 2009; Gyebi L et al. Curr Hypertens Rep 2012]. Subgroup analyses in patients with CKD from prior statin studies demonstrated that the benefits of statin therapy extended to patients with CKD. Indeed, there was a 14.5% decline in total mortality (p=0.045) in the Pravastatin Pooling Project [Tonelli M et al. Circulation 2004]. The landmark Study of Heart and Renal Protection [SHARP] trial found that reduction of LDL cholesterol with simvastatin 20 mg in combination with ezetimibe 10 mg daily safely reduced the incidence of major atherosclerotic events in a wide range of patients with advanced CKD, including those managed with dialysis as well as patients not requiring dialysis [Baigent C et al. Lancet 2011] (Figure 2).

Reduced LDL Cholesterol Cut the Incidence of Major Atherosclerotic Events in Advanced CKD Patients.
LDL=low-density lipoprotein.
Reprinted with permission from The Lancet 2011. Baigent C et al. The effects of lowering cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease.
Future research will focus on reducing the risk of acute renal failure, defining optimal revascularization and reperfusion strategies, reducing bleeding, and the assessment and treatment of nontraditional CKD-related risk factors (eg, anemia, brain natriuretic peptide, parathyroid hormone, calcium, phosphorus, homocysteine, inflammation, thrombotic factors, and oxidative stress).
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.