

Summary
Peripheral artery disease (PAD) affects an estimated 27 million individuals in Europe and North America [Owens CD, Conte MS. Circulation 2012]. It has high morbidity and mortality even if asymptomatic [Leng GC et al. Int J Epidemiol 1996]. This article discusses the diagnosis and treatment of PAD.
- Hypertensive Disease
Peripheral artery disease (PAD) affects an estimated 27 million individuals in Europe and North America [Owens CD, Conte MS. Circulation 2012]. It has high morbidity and mortality even if asymptomatic [Leng GC et al. Int J Epidemiol 1996]. Matthews Chacko, MD, Johns Hopkins University, Baltimore, Maryland, USA, discussed the diagnosis and treatment of PAD.
He reviewed the etiology, epidemiology, and demographic features of PAD; the importance of the ankle brachial index (ABI); the assessment of cardiovascular (CV) risk; and management of patients with PAD, in particular those from the Caribbean nations. Previous studies have indicated that African Caribbeans report more distal PAD than the general population [Bennett PC et al. Q J Med 2009].
PAD is a manifestation of generalized atherosclerosis and, therefore, an independent predictor of CV ischemic events [Leng GC et al. BMJ 1996; Criqui MH et al. N Engl J Med 1992]. Bennet et al. [Q J Med 2009] report that its presence is associated with an increased risk of cerebrovascular disease and coronary artery disease (CAD); that people with PAD have a 4 to 5 times greater risk of dying from a CV disease event compared with those without it, and a 2 to 3 times greater risk of all-cause mortality.
Although risk factors for CAD and PAD overlap [Bhatt DL et al. JAMA 2006], patients with PAD are less likely to receive optimal medical therapy than those with CAD. The majority of those with PAD are either asymptomatic or have atypical leg symptoms, with classical claudication in only 10% to 35% of affected individuals. Therefore, detection is elusive unless actively sought [Owens CD. Circulation 2012].
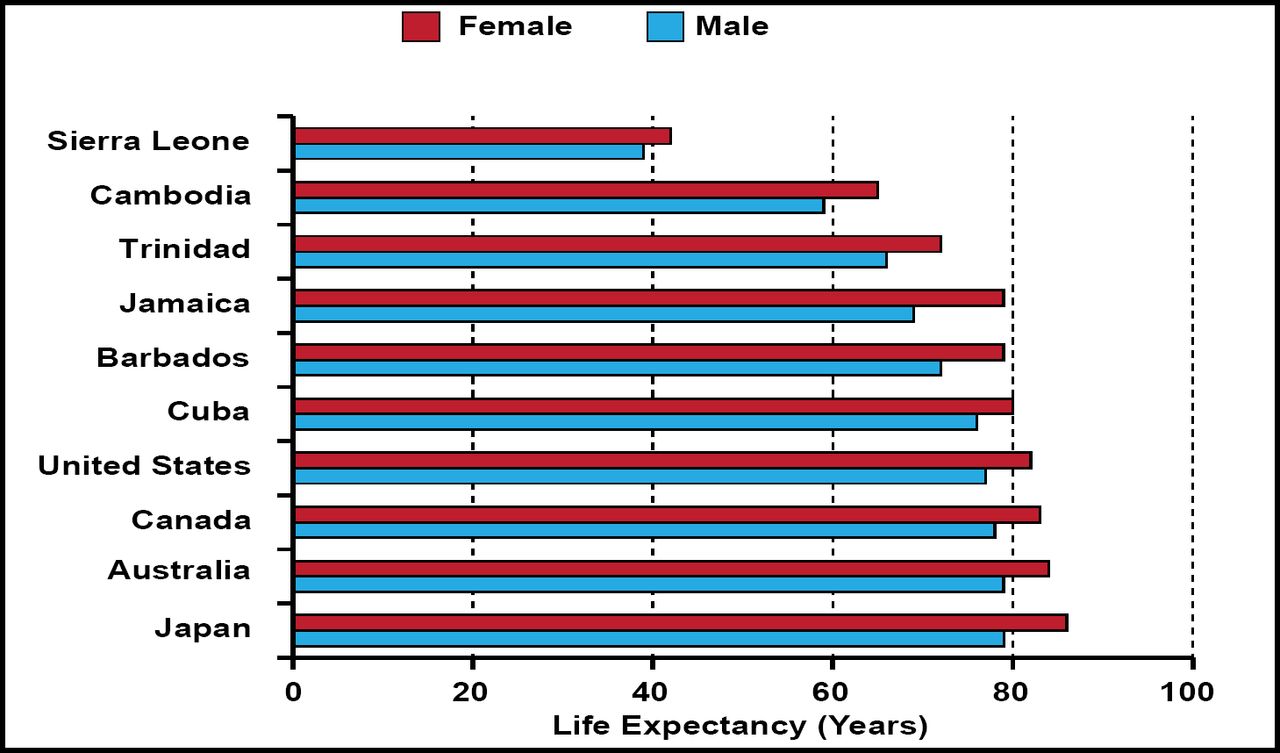
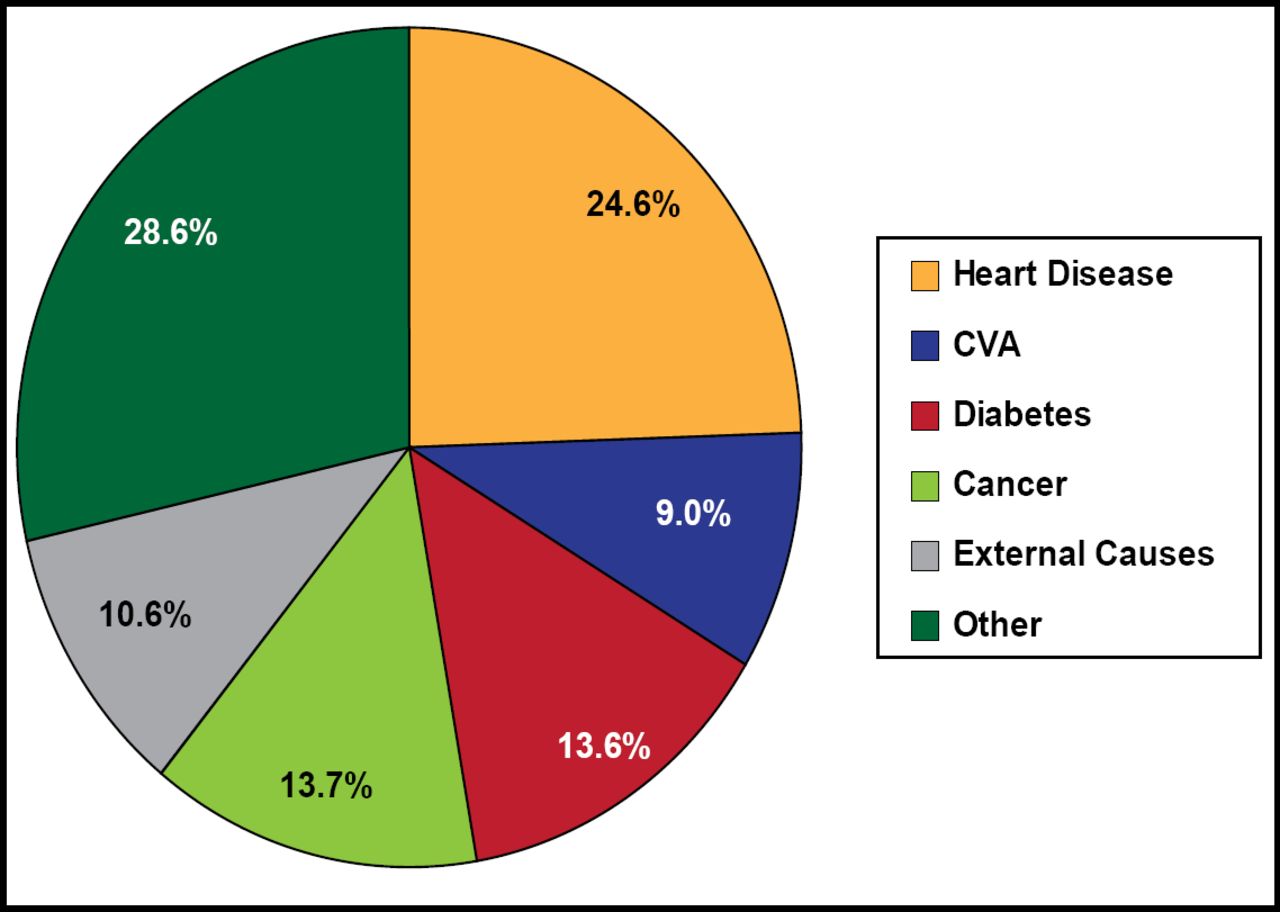
According to Dr. Chacko, PAD patients may have CAD, carotid disease, or abdominal aortic aneurysm. A “panvascular” focus is mandatory to optimize patient outcomes, along with early recognition of the disease, the initiation of appropriate medical treatment, and assessment for revascularization. The need is especially great in the Caribbean where life expectancy is shorter than it is in other nations (Figure 1). In Trinidad and Tobago, heart disease was the leading cause of death, accounting for 24.6% of all deaths in 2006 (Figure 2).

Life Expectancy by Nation in 2006.
Reproduced with permission from M. Chacko, MD.

Causes of Death in Trinidad and Tobago in 2006.
CVA=cerebrovascular accident.
Reproduced with permission from M. Chacko, MD.
Hirsch et al. [JAMA 2001] report that the prevalence of PAD in primary care practices is high, yet physician awareness of the diagnosis is relatively low. They found that measurement of a simple ABI identified a large number of patients with previously unrecognized PAD. Owens and Conte [Circulation 2012] report that clinical history and electrocardiogram detect only 20% to 40% of coexisting disease whereas cardiac catheterization identifies CAD in as many as 90% of PAD patients.
“CAD is just the tip of the atherosclerotic iceberg,” said Dr. Chacko, adding that PAD is a common and a poor prognostic marker. He cited a critical need for increased awareness, with early diagnosis and medical therapy. He also said that stopping smoking and walking are vital in the management of PAD and its related CV comorbidities.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.