

Summary
Significant advances have been made in the recognition and diagnosis of hypertension, but many patients have not achieved blood pressure control at levels that reduce cardiovascular risk. This article discusses the current state of antihypertensive therapy, compliance, and angiotensin receptor blockers.
- Hypertensive Disease
Blood Pressure Control
Significant advances have been made in the recognition and diagnosis of hypertension, but many patients have not achieved blood pressure (BP) control at levels that reduce cardiovascular (CV) risk. Marcelo Orías, MD, Sanatorio Allende, Córdoba, Argentina, discussed the current state of antihypertensive therapy.
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) [Chobanian AV et al. JAMA 2003] and European Society of Hypertension-European Society of Cardiology (ESH-ESC) guidelines [J Hypertens 2003] define hypertension as systolic BP (SBP) of ≥140 mm Hg and/or diastolic BP (DBP) of ≥90 mm Hg for an extended time. For individuals with diabetes mellitus, kidney disease, or other high-risk conditions such as stroke or myocardial infarction (MI), the guidelines recommend a target BP of <130/80 mm Hg.
The Framingham study showed that the relative risk of stroke and coronary heart disease increases as BP increases. Vasan et al. [N Engl J Med 2001] demonstrated increased cumulative incidence of CV events as SBP increases from optimal (<120 mm Hg) to normal (121–129 mm Hg) to high-normal DBP (130–139 mm Hg). In the Hypertension Optimal Treatment [HOT] study, the incidence of major CV events was similar in individuals with DBP ≤80 mm Hg, ≤85 mm Hg, and ≤90 mm Hg but there was a significant difference in the number of major CV events in patients with diabetes with target DBP ≤90 versus ≤85 versus ≤80 (24.4 vs 18.6 vs 11.0 per 1000 patient-years; p=0.005 for trend) [Hansson L et al. Lancet 1998].
The Action to Control Cardiovascular Risk in Diabetes [ACCORD] Study Group [N Engl J Med 2010] reported that patients with diabetes receiving intensive antihypertensive therapy had an average SBP of 119.3 mm Hg compared with 133.5 mm Hg in diabetes patients on standard therapy. Most CV outcomes were not significantly different between the 2 groups but stroke was significantly higher in the standard therapy (0.53% per year) versus the intensive therapy group (0.32% per year; HR, 0.59; 95% CI, 0.39 to 0.89; p=0.01). However, evidence of benefit from more active treatment in diabetic patients is inconsistent across trials [ESH/ESC Guidelines. J Hypertens 2009].
Essential hypertension probably is caused by a combination of mechanisms, some of which are more important in some patients than others. The ESH/ESC algorithm for treatment of hypertension recommends customizing the choice of therapy to the individual patient and initiating treatment with a low-dose single agent or low-dose combination of 2 agents [ESH/ESCGuidelines. J Hypertens 2009]. The JNC 7 treatment algorithm recommends lifestyle changes, followed by pharmacologic therapy if BP targets are not reached [Chobanian AV et al. JAMA 2003]. The updated UK National Institute for Clinical Excellence (NICE) recommendations for antihypertensive therapy are shown in Figure 1.

Updated UK NICE Guidelines for the Treatment of Newly Diagnosed Hypertension.
ACEI=angiotensin-converting enzyme inhibitors; ARB=angiotensin receptor blockers; CCB=calcium channel blocker. Source: NICE Clinical Guideline 127.2011. www.nice.org.uk/guidance/CG12.
Compliance
Analysis of the third National Health and Nutrition Examination Survey found that of the 41.9 million people in the United States with hypertension, 31% were unaware they had hypertension, 17% were aware but not receiving treatment, 29% were being treated but remained uncontrolled, and 23% who were being treated had achieved control to <140/90 mm Hg [Hyman DJ & Pavlik VN. N Engl J Med 2001]. In persons aged ≥65 years, 45% were unaware of their condition, 32% were aware of their hypertension but were not receiving treatment, and 57% had treated but uncontrolled hypertension.
Halpern et al. [J Hypertens 2006] found that patients with increased compliance and persistence with antihypertensive therapy after reaching the BP goal had reduced their predicted relative risk (men, 4.6%; women, 16.4%) and absolute risk (2.1%) of adverse CV outcomes. A retrospective analysis (n=137,277) showed that patients with high adherence (80% to 100%) had a significantly decreased risk of hospitalization (27%) compared to those with compliance of 1% to 19% (44%), 20% to 139% (39%), 40% to 159% (36%), and 60% to 179% (30%) [Sokol MC et al. Med Care 2005]. Another retrospective analysis showed that ≥80% compliant patients used fewer outpatient resources than <80% compliant patients [Halpern Value Health 2005]. Mancia et al. [ESC 1999] showed that 53.3% of patients change their antihypertensive therapy because of adverse effects and 34.1% because their BP was not controlled. Burke et al. [J Hypertens 2006] found that persistence with antihypertensive therapy substantially declines within the first year of treatment.
Angiotensin Receptor Blockers
Angiotensin receptor blockers (ARBs) have been studied extensively. The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial [ONTARGET] investigators randomized 25,620 high-risk patients to telmisartan, ramipril, or telmisartan plus ramipril [ONTARGET Investigators. N Engl J Med 2008]. The primary composite endpoint of CV death, MI, stroke, or hospitalization for heart failure occurred in 16.5% of the ramipril group and in 16.7% of the telmisartan group, showing that the ARB telmisartan was as effective as angiotensin converting enzyme inhibitor (ACE-I) ramipril for reducing the risk of CV events. Telmisartan was associated with lower rates of cough (1.1% vs 4.2%; p<0.001) and angioedema (0.1% vs 0.3%; p=0.01).
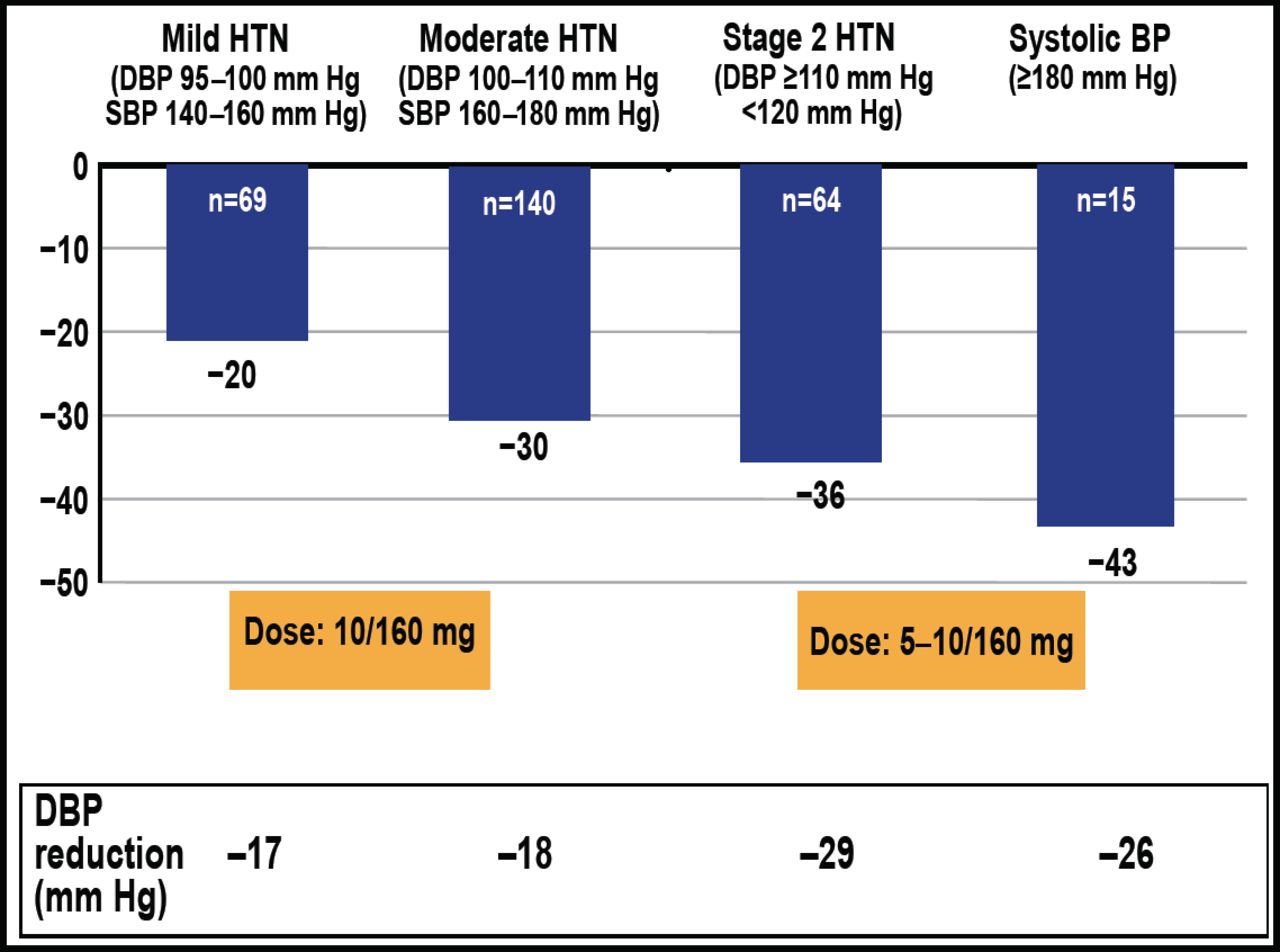
In the Co-Valsartan Initial Therapy Trial [CDITT], patients treated with valsartan (ARB acting on the AT1 receptor) plus hydrochlorothiazide achieved greater BP control versus those treated with valsartan alone (39.6% vs 21.8%; p<0.0001) [Calhoun DA et al. Curr Med Opin Res 2008]. Jackson et al. [Value Health 2006] showed that patients receiving fixed-dose therapy with valsartan/hydrochlorothiazide had greater persistence with therapy than those treated with a free combination of valsartan plus hydrochlorothiazide (54% vs 19%; p<0.0001). Studies of amlodipine/valsartan have shown that appropriate BP reductions occur across all grades of hypertension, with greater decreases as BP severity increases (Figure 2).

Amlodipine/Valsartan: Appropriate BP Reductions across All Grades of Hypertension.
BP=blood pressure; DBP=diastolic blood pressure; HTN=hypertension; SBP=systolic blood pressure; Reproduced with permission from M. Orias, MD.
Combining a calcium channel blocker (CCB) with an ARB reduces the edema associated with CCBs. The Avoiding Cardiovascular Events through Combination Therapy in Patients Living with Systolic Hypertension [ACCOMPLISH] trial compared initial therapy with the single-pill combination of a renin-angiotensin-aldosterone system blocker (benazepril) and a CCB (amlodipine) versus benazepril/hydrochlorothiazide in high-risk hypertensive patients [Jamerson K et al. N Engl J Med 2008]. The primary endpoint was the composite of CV morbidity and mortality. This primary event occurred in 552 patients (9.6%) in the benazepril/amlodipine group versus 679 patients (11.8%) in the benazepril/hydrochlorothiazide group, for a relative risk reduction of 19.6% (HR, 0.80; 95% CI, 0.72 to 0.90; p<0.001).
A large proportion of patients require >2 antihypertensive agents to achieve BP control, as shown in the United Kingdom Prospective Diabetes Study [UKPDS; 27% to 31%], Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial [ALLHAT; 23%], and ACCOMPLISH (26%) trials [UKPDS. BMJ 1998; Cushman WC et al. J Clin Hypertens 2008; Jamerson K et al. Blood Press 2007]. Calhoun et al. [Hypertension 2009] showed that SBP reductions were greater with triple-combination therapy with amlodipine/valsartan/hydrochlorothiazide (−39.7 mm Hg) versus valsartan/hydrochlorothiazide (−32.0 mm Hg), amlodipine/valsartan (−33.5 mm Hg), and hydrochlorothiazide/amlodipine (−31.5 mm Hg; p<0.0001). The triple combination was well tolerated, with similar adverse event (AE) rates across all treatment groups (44.9% to 48.3%). AEs were as expected, mostly mild and transient with no indication of target organ toxicity.
Dr. Orías concluded that AT1 blockers are as potent as and better tolerated than ACE-I. Furthermore, since fixed-dose combination therapy including an AT1 blocker has good compliance, it represents a highly desirable regimen for patients that require more than one antihypertensive agent to achieve their BP goals.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.