

Summary
The use of fractional flow reserve (FFR) has helped interventional cardiologists gain a better understanding of coronary artery obstruction. This article discusses the physiology of FFR and the United Kingdom experience, as well as the Trinidad and Tobago experience with FFR.
- Coronary Artery Disease Interventional Techniques & Devices
The use of fractional flow reserve (FFR) has helped interventional cardiologists gain a better understanding of coronary artery obstruction. Huon H. Gray, MD, Department of Health, London, United Kingdom (UK), discussed the physiology of FFR and the UK experience. In the second presentation, Ronald Henry, MD, Advanced Cardiovascular Institute, Port of Spain, Trinidad and Tobago, West Indies, talked about the Trinidad and Tobago experience with FFR.
Physiology, Evidence, and UK Experience
Prof. Gray commented that angiography has a number of limitations. Modern angiographic equipment resolves only about 5 line pairs/mm and structures <0.2 mm cannot be visualized. Motion artifact is another issue. Most importantly, angiographic interpretation of the severity of coronary stenosis often correlates poorly with the degree of myocardial ischemia.
The presence and extent of inducible ischemia is the most important predictor of outcome in patients with a similar degree of anatomic disease. Regardless of the angiogram appearance, the functional consequences of atheroma should be addressed, particularly the presence of blood flow limitation. FFR can help cardiologists determine whether an angiographically significant lesion is causing ischemia. FFR is determined using a guide wire that can accurately measure blood pressure proximal and distal to a coronary stenosis under conditions of maximal coronary hyperemia induced with adenosine. FFR is calculated as the relationship between pressure distal to a stenosis with pressure proximal to the stenosis during maximal hyperemia.
Several studies have shown that the predictive accuracy of FFR at a threshold value of ∼0.75 (normal, 1.0) compared with noninvasive tests of ischemia ranges from 80% to 96%. At FFR ≥0.80, noninvasive stress testing is negative for inducible ischemia. Advantages of FFR include the following: it has an unequivocal normal value of 1.0, it can be obtained during angiography and percutaneous coronary intervention (PCI) can follow immediately, it is independent of hemodynamic conditions, it accounts for collateral circulation; it is highly reproducible, and it is applicable to multivessel disease (MVD).
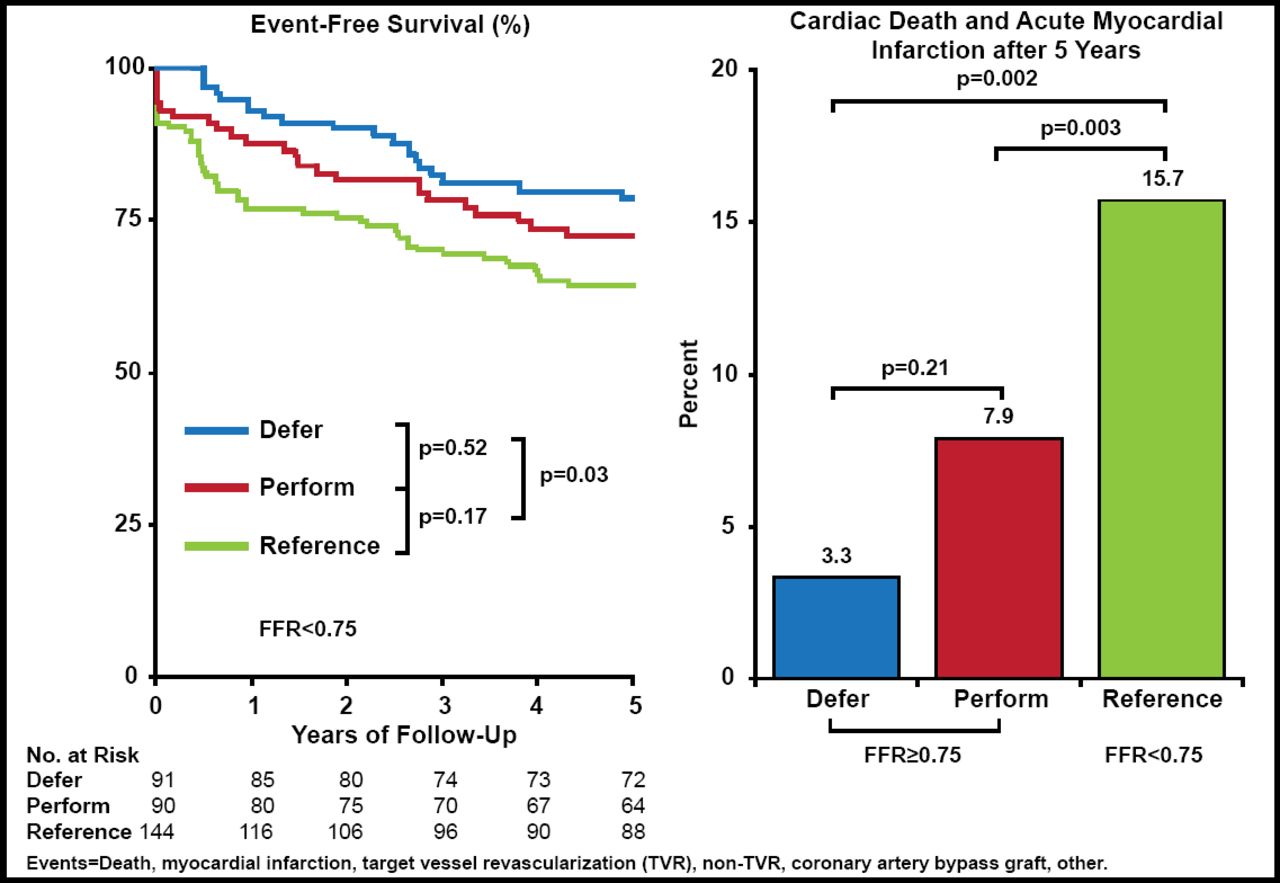
The Deferral of Percutaneous Coronary Intervention [DEFER] study evaluated FFR in patients with single vessel disease (SVD) and stable chest pain [Pijls NHJ et al. J Am Coll Cardiol 2007]. Patients scheduled for single-vessel PCI without prior proof of ischemia (n=325) were randomized to a “Defer PCI” or “Perform PCI” strategy for those with an FFR of >0.75. Those with FFR <0.75 had PCI undertaken and were entered into a registry (reference group). At 5 years, event-free survival was similar between the Defer (80%) and Perform (73%) groups (p=0.52) but was significantly worse in the Reference group (63%; p=0.03 vs Defer and Perform; Figure 1). The cardiac death and acute myocardial infarction (MI) composite rate was lower in the Defer (3.3%) and Perform (7.9%) versus Reference (15.7%) group (Defer vs Reference; p=0.002; Defer and Perform vs Reference; p=0.003). This study showed that it is safe to not perform PCI in patients with stable angina and angiographically significant single vessel disease when FFR >0.75.

DEFER Study: 5-Year Data.
Reprinted from J Am Coll Cardiol 2007;49(21):2015. Pijls NJH et al. Percutaneous coronary intervention of functionally nonsignificant stenosis; with permission from Elsevier.
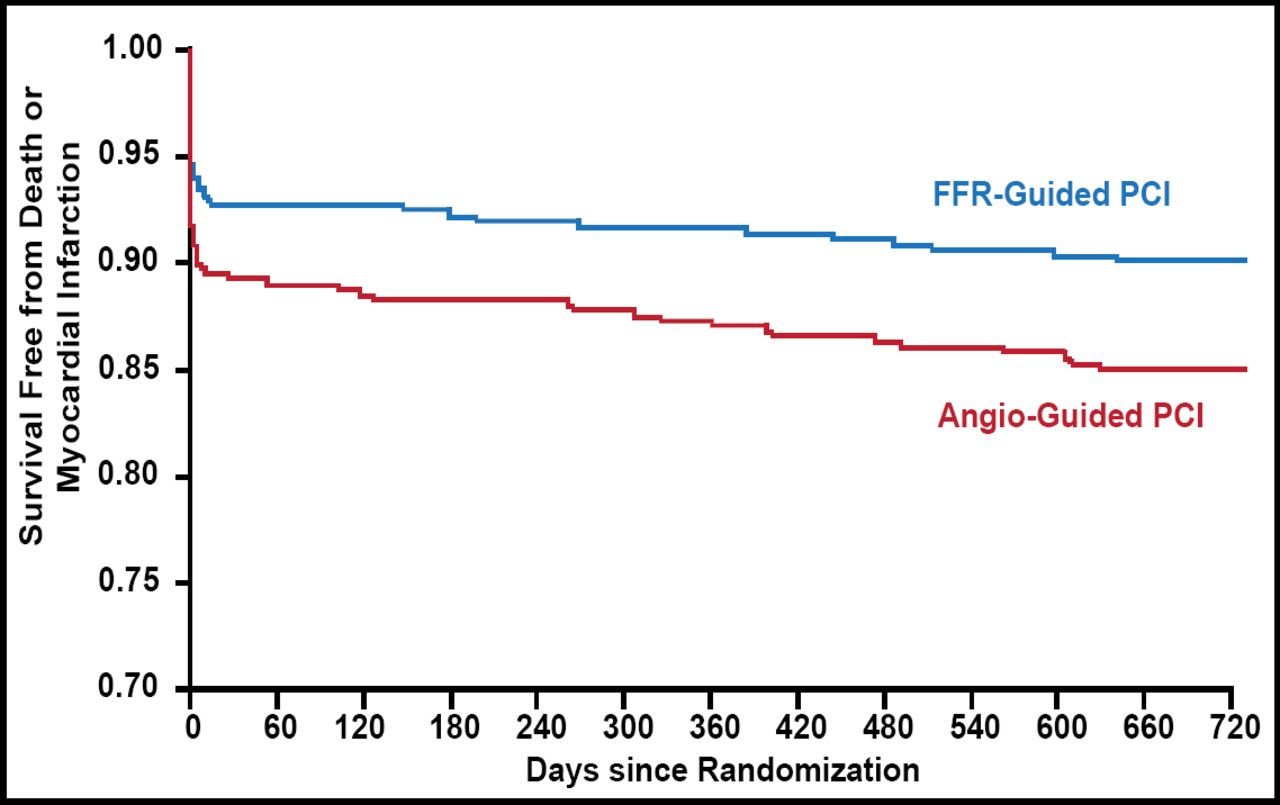
Several studies have evaluated FFR in patients with multivessel coronary disease. The Fractional Flow Reserve versus Angiography for Multivessel Evaluation [FAME] study randomized patients to angiography-guided PCI with drug-eluting stent (DES) on all indicated lesions versus FFR-guided PCI with DES performed on indicated lesions if FFR was ≤0.80 [Pijls NHJ et al. J Am Coll Cardiol 2010]. The 2-year composite of mortality and MI rates was 12.9% with angiography-guided PCI versus 8.4% with FFR-guided PCI (p=0.02; Figure 2). The results were therefore similar to DEFER, showing that it is safe not to undertake PCI for lesions with an FFR>0.8 in patients with stable multivessel disease

FAME Study: 2-Year Results.
Reprinted from J Am Coll Cardiol 2010;55(25):2816. Pijls NJH et al. Functional severity of coronary artery stenoses in the FAME study; with permission from Elsevier.
The 2010 European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) Guidelines on myocardial revascularization recommends FFR-guided PCI for detection of ischemia-related lesions when objective evidence of vessel-related ischemia is not available (based on DEFER and FAME evidence) [Wijns W et al. Eur Heart J 2010]. The 2011 American College of Cardiology Foundation/American Heart Association/Society for Cardiovascular Angiography and Interventions Guideline for Percutaneous Coronary Intervention states that FFR is reasonable to assess angiographic intermediate coronary lesions and can be useful for guiding revascularization decisions in patients with stable ischemic heart disease [Levine GN et al. Circulation 2011]. In the United Kingdom, the number of PCI procedures has increased from 174 per million people in 1991 to 87,676 per million in 2010. In 2010, pressure wire procedures accounted for 10.4% of all PCI in the United Kingdom [http://www.bcis.org.uk/pages/page_box_contents.asp?PageID=746].
Prof. Gray concluded that the evidence base for FFR is now strong but stressed that the data published to date refers to its use in patients with stable coronary disease. Further work is needed to determine the place of FFR in the management of patients with acute coronary syndromes (ACS).
The Trinidad and Tobago Experience
The Advanced Cardiovascular Institute in Trinidad and Tobago began using FFR in June 2010. From January to June 2012, 136 PCI and 7 FFR procedures (5%) were performed, which is comparable to the 5% to 8% FFR rate in Europe. According to Dr. Henry, reasons for the low FFR rate include the following: some patients present with ischemia with 1 lesion, which is stented; others have ST-segment elevation MI with 1 culprit artery, for which FFR has not been validated; and some guidelines recommend coronary artery bypass graft (CABG) for MVD.
Issues with FFR adoption include the need for an add-on guide catheter, increased per-case cost of FFR add-on to diagnostic catheterization in private sector laboratories (although public institutions save money by avoiding stenting in some patients), negative referral bias when the diagnostic angiographer and interventionist are different persons, and longer procedure time.
Dr. Henry briefly reviewed the results and implications of the FAME II study. This study evaluated FFR in patients with stable coronary artery disease (CAD) post angiogram referred for PCI and included both randomized and registry cohorts. The randomized cohort included 1219 patients with FFR-positive 1-, 2-, or 3-vessel disease. The registry cohort included 166 patients who were angiogram-positive but FFR-negative. The 812 FFR-positive patients were randomized 1:1 to optimal medical therapy (OMT) versus OMT plus DES; the 131 FFR-negative patients received OMT. At 1-year follow-up, the urgent revascularization rate was 0.6% in the FFR-negative OMT-only group, 6% in the FFR-positive OMT-only group, and 0.6% in the FFR-positive OMT plus DES group [Pijls NHJ et al. J Am Coll Cardiol 2010]. Thus, although the 2007 Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation [COURAGE] trial showed that OMT is effective in angiographically severe but clinically stable CAD [Boden WE et al. N Engl J Med 2007], FAME II showed that OMT is not effective in FFR-positive patients.
After describing some successful FFR case studies from ACI, Dr. Henry concluded that FFR is an important tool for selected cases in the Trinidad region. The potential exists for wide application for cost reduction in state laboratories. Further research is needed on FFR/DES versus CABG and FFR-guided nonculprit vessel intervention in patients with ACS.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.