

Summary
Approximately two-thirds of patients with systemic sclerosis develop interstitial lung disease (ILD). High-resolution computed tomographyof the chest is the gold standard for diagnosing ILD, but it cannot be used often because of the risks that are associated with radiation exposure and cost concerns. Recent data have suggested that lung ultrasound can aid in the detection of ILD by evaluating B-lines, the sonographic marker of pulmonary interstitial syndrome.
- Rheumatological Autoimmune Disorders Clinical Trials
Approximately two-thirds of patients with systemic sclerosis develop interstitial lung disease (ILD). High-resolution computed tomography (HRCT) of the chest is the gold standard for diagnosing ILD, but it cannot be used often because of the risks that are associated with radiation exposure and cost concerns. Recent data have suggested that lung ultrasound (LUS) can aid in the detection of ILD by evaluating B-lines, the sonographic marker of pulmonary interstitial syndrome. The aims of this study [Barskova T et al. Ann Rheum Dis 2012] were to verify the correlation between HRCT detection of ILD and B-lines and to evaluate the reliability of LUS as a screening tool in patients with very early systemic sclerosis.
A total of 58 consecutive patients (54 women, mean age 51±14 years) with systemic sclerosis were evaluated with chest HRCT and LUS. LUS was performed on the right and left hemithoraces to evaluate the location and number of B-lines. A B-line was defined as an echogenic coherent wedge-shaped signal with a narrow origin in the near field of the image [Volpicelli et al. Intensive Care Med 2012]. The number of B-lines in the intercostal spaces was recorded and totaled to produce a score that denoted the extent of ILD. ILD was diagnosed when ≥3 B-lines were found in at least 2 adjacent scanning sites or when >5 B-lines were present.
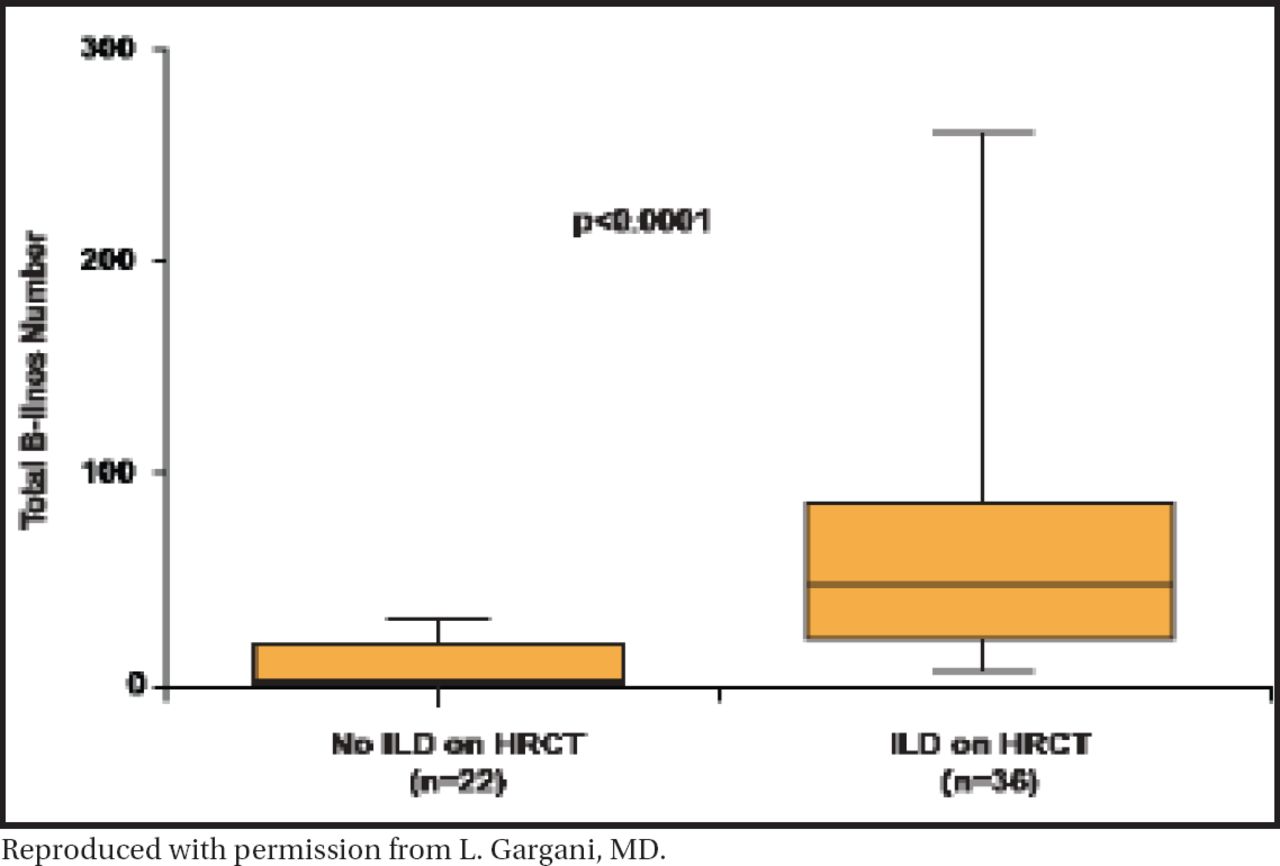
Among the total population, 32 patients (29 women, mean age 51±15 years) were diagnosed with very early systemic sclerosis. HRCT and LUS were performed a mean of 42±46 days (median 27 days) apart. ILD was found on HRCT in 88% of the total population and in 41% of the very early systemic sclerosis population (p<0.01). Significantly more B-lines were found in patients with HRCT-detected ILD (mean 57±53, median 43) versus those without (mean 9±9, median 5; p<0.0001; Figure 1). Patients with ground glass on HRCT (n=13; 63±47) had a higher total number of B-lines than patients without ground glass (33±40; p<0.05). There was no statistically significant difference in the number of B-lines that were detected between younger (≤50 years) and older (>50) patients or between patients with shorter (<1 year) or longer (>1 year) disease duration.

Difference in Number of B-Lines in Patients With and Without ILD on HRCT.
Reproduced with permission from L. Gargani, MD.
Analysis of individual patients in the overall population showed 83% concordance between LUS and HRCT, with 100% sensitivity, 100% negative predictive value, 55% specificity, and 78% positive predictive value. All 10 discordant cases were false positive on LUS. Receiver operating characteristic (ROC) curve analysis confirmed the analytical relationship between the number of B-lines and the presence of ILD on HRCT (area under curve, 0.94; 95% CI, 0.89 to 0.99; p<0.0001). The presence of >5 B-lines had 100% sensitivity and 59% specificity. The presence of ≥20 B-lines had 83% sensitivity and 96% specificity.
This study shows that LUS is highly sensitive for detecting ILD in patients with very early systemic sclerosis. The presence of B-lines on LUS examination correlates with detection of ILD on HRCT. LUS appears to be a reliable screening tool to determine which patients should be evaluated further with HRCT.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.