

Summary
This article revisits the 2003 JNC 7 guidelines, as well as newer evidence regarding the use of renin-angiotensin system (RAS) inhibitors, calcium channel blockers, and diuretics to treat patients with diabetes and hypertension. The American Diabetes Association issued new guidelines in 2012 to address some of the recent controversy concerning the use of antihypertensive agents in patients with diabetes and to provide additional recommendations concerning the use of RAS inhibitors. These recommendations were based on evidence from a number of clinical trials.
- Renal Disease
- Diabetes & Kidney Disease
- Diabetes & Endocrinology Guidelines
- Diabetes Mellitus
- Hypertensive Disease
- Hypertension & Kidney Disease
While anticipating the new Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC) 8 guidelines, Suzanne Oparil, MD, University of Alabama, Birmingham, Alabama, USA, revisited the 2003 JNC 7 guidelines, as well as newer evidence regarding the use of renin-angiotensin system (RAS) inhibitors, calcium channel blockers (CCBs), and diuretics to treat patients with diabetes and hypertension.
The American Diabetes Association (ADA) issued new guidelines in 2012 to address some of the recent controversy concerning the use of antihypertensive agents (Table 1) in patients with diabetes and to provide additional recommendations concerning the use of RAS inhibitors. These recommendations were based on evidence from a number of clinical trials. Dr. Oparil discussed the United Kingdom Prospective Diabetes Study [UKPDS; Holman RR et al. N Engl J Med 2008] and the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial [ALLHAT; ALLHAT Collaborative Research Group. JAMA 2003] in detail. In the UKPDS, 758 patients with type 2 diabetes were randomly assigned to the angiotensin-converting enzyme (ACE) inhibitor (captopril) or a β-blocker (atenolol). There were no differences in blood pressure (BP) control, in diabetes-related or cardiovascular disease (CVD)-related endpoints, or in renal outcomes between the two treatment groups.
RAS Inhibitor Guidelines.
In the ALLHAT study, 33,357 patients with hypertension, 12,063 of whom had diabetes, were randomly assigned to either a diuretic (chlorthalidone), a CCB (amlodipine), or an ACE inhibitor (lisinopril). CVD and end-stage renal disease (ESRD) events were similar in participants with and without diabetes. Compared with the diuretic arm, there was a higher risk of heart failure with amlodipine and a higher risk of stroke, heart failure, and combined CVD with lisinopril. Dr. Oparil cautioned that ALLHAT did not address patients with chronic kidney disease (CKD) or proteinuric nephropathy. To address this shortcoming, she discussed results of 2 studies that examined the effects of angiotensin II receptor blockers (ARBs) on the incidence of diabetic nephropathy. In the Irbesartan in Patients with Type 2 Diabetes and Microalbuminuria [IRMA 2; Parving HH et al. N Engl J Med 2001] study, adding an ARB (irbesartan) to conventional antihypertensive therapy significantly (p=0.001) reduced the incidence of diabetic nephropathy and decreased the amount of urinary albumin. The Reduction of Endpoints in Non-Insulin Dependent Diabetes With the Angiotensin II Antagonist Losartan [RENAAL; Brenner BM et al. N Engl J Med 2001] trial was a double-blind, placebo-controlled trial to evaluate the renal-protective effects of losartan in patients with type 2 diabetes with nephropathy. Losartan reduced proteinuria, delayed onset of the primary endpoint (doubling of serum creatinine/ESRD/death), slowed the rate of decline in renal function, delayed progression to ESRD, and lowered BP by an additional 3/1 mm Hg. The results from these 2 studies led to the adoption of the Kidney Disease: Improving Global Outcomes (KDIGO) recommendations (Table 2).
KDIGO Recommendations.
Dr. Oparil had 3 key messages for physicians:
-
Evidence for selecting any one drug class for initial treatment of patients with diabetes and hypertension is sparse except in the presence of CKD with proteinuria
-
Initial drug therapy for patients with diabetes, hypertension, and CKD with proteinuria should be an ACE inhibitor or an ARB
-
Most patients with diabetes and hypertension will require more than one antihypertensive drug to achieve BP goal
Peter M. Nilsson, MD, Lund University, Malmö, Sweden, argued for more flexible goals to control hypertension in patients with diabetes. Randomized controlled trials and observational studies have shown either no benefit or even harm for increased coronary heart disease (CHD) risk that is associated with intensive systolic blood pressure (SBP) control <130 mm Hg.
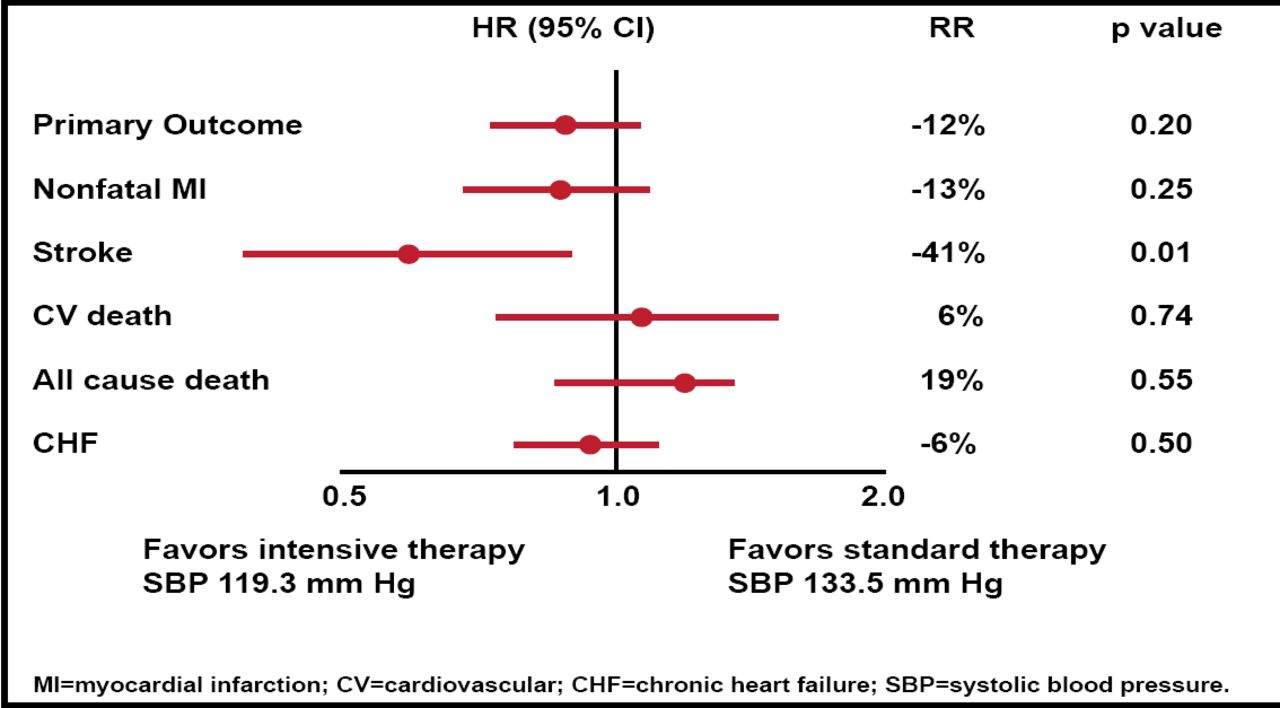
Results from major trials show that it is difficult to reduce BP below 130 mm Hg in patients with type 2 diabetes mellitus (T2DM) [Mancia G et al. J Hypertens 2009], and even when BP is reduced to very low levels, results suggest that, except for stroke, there is little reduction in primary cardiovascular outcomes or mortality (Figure 1) [Zanchetti A. Eur Heart J 2010; Cushman W et al. N Engl J Med 2010].

ACCORD-BP: Primary and Secondary Outcomes.
Reproduced with permission from PM Nilsson, MD.
In a reappraisal of European guidelines, the European Society of Hypertension (ESH) recommends using a flexible BP goal in individuals with diabetes. In newly detected T2DM, the goal should be tighter risk factor control; in elderly patients with a long duration of diabetes and many comorbidities, a more flexible goal is recommended; patients should be treated when hypertension is ≥140/90 mm Hg or lower if signs of target organ damage are present. Use 24-hour ambulatory BP measurement to detect masked hypertension in normotensive T2DM patients. The European Guidelines on Cardiovascular Disease Prevention in Clinical Practice [Perk J et al. Eur Heart J 2012] recommend treating targets of <140/80 mm Hg (Class I, Level A), while the 2011 ADA Standard of Medical Care in Diabetes [Diabetes Care 2011] recommends a goal of SBP <130 mm Hg (Level C) and diastolic blood pressure (DBP) <80 mm Hg (Level B); however, the recommendations note that higher or lower SBP targets may be appropriate, based on a patient's characteristics and response to therapy (Level B) [Diabetes Care 2012 Suppl]. Level of Evidence C is given for the SBP goal, which is considered low. The ADA's view is gradually shifting to be more in line with that of the ESH and the European Society of Cardiology.
Prof. Nilsson presented results from a recent study [Redon J et al. J Am Coll Cardiol 2012] that showed that the relationship between BP and overall cardiovascular risk had a similar pattern in patients with and without diabetes over a wide range of baseline and in-treatment BP values, although, for the same SBP, a higher risk was observed in patients with diabetes. Other evidence [Cederholm J et al. J Hypertens 2010] suggests the risks of CHD and stroke increased progressively with higher SBP, with no J-shaped curves, although the risk increase was significant only for SBP of at least 140 mm Hg, but did not compare 130 mm Hg to 139 mm Hg and 110 mm Hg to 129 mm Hg. In addition, baseline SBP of 110 mm Hg to 129 mm Hg showed increased CHD and CVD risk with further SBP reduction during follow-up, whereas baseline SBP of at least 130 mm Hg showed benefits. Thus, some patients with CHD might be at risk if SBP is reduced below 110 mm Hg.
Observational data from a meta-analysis of 13 randomized trials [Bangalore S et al. Circulation 2011] concluded that an SBP treatment goal of 130 mm Hg to 135 mm Hg is acceptable in patients with T2DM and impaired glucose control. With more aggressive goals (<130 mm Hg), although the risk of stroke continued to decrease, there was no benefit regarding the risk of other macrovascular or microvascular (cardiac, renal, and retinal) events, and the risk of serious adverse events increased.
Newer guidelines are emerging that state the BP goal for most individuals is <140/90 mm Hg (Level IA or IB) and levels <130/80 mm Hg are defensible only if advanced proteinuric CKD is present or if the risk of stroke is high [Flynn C, Bakris GL. Curr Hypertens Rep 2011].
Prof. Nilsson concluded that diabetes is associated with increased cardiovascular risk, and a multiple risk factor control approach is needed. Although drug combinations may be necessary, he suggested that physicians should beware of combining ACE inhibitors and angiotensin receptor blockers (ARB) solely for the treatment of hypertension because of the possibility of side effects. The use of a triple combination of an ACE inhibitors + ARB/direct renin inhibitor should also be avoided, based on data from the Aliskiren Trial in Type 2 Diabetes Using Cardiovascular and Renal Disease Endpoints [ALTITUDE; NCT00549757], showing no benefit and, in fact, an increase in adverse events, especially nonfatal stroke. Use loop diuretics if renal impairment is present and b-blockers if CHD is present.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.