

Summary
Diabetes affects 25.8 million people of all ages, or 8.3% of the US population. In 2007, it was the seventh leading cause of death. More than 60% of nontraumatic lower limb amputations occur in people with diabetes. In 2006, that number totaled approximately 65,700 [National Diabetes Information Clearinghouse (NDIC) National Diabetes Fact Sheet 2011]. This article discusses nonoperative management of the infected diabetic foot.
- Diabetes Mellitus
Diabetes affects 25.8 million people of all ages, or 8.3% of the US population. In 2007, it was the seventh leading cause of death. More than 60% of nontraumatic lower limb amputations occur in people with diabetes. In 2006, that number totaled approximately 65,700 [National Diabetes Information Clearinghouse (NDIC) National Diabetes Fact Sheet 2011]. During an interactive case-based session, John M. Embil, MD, University of Manitoba, Winnipeg, Manitoba, Canada, discussed nonoperative management of the infected diabetic foot.
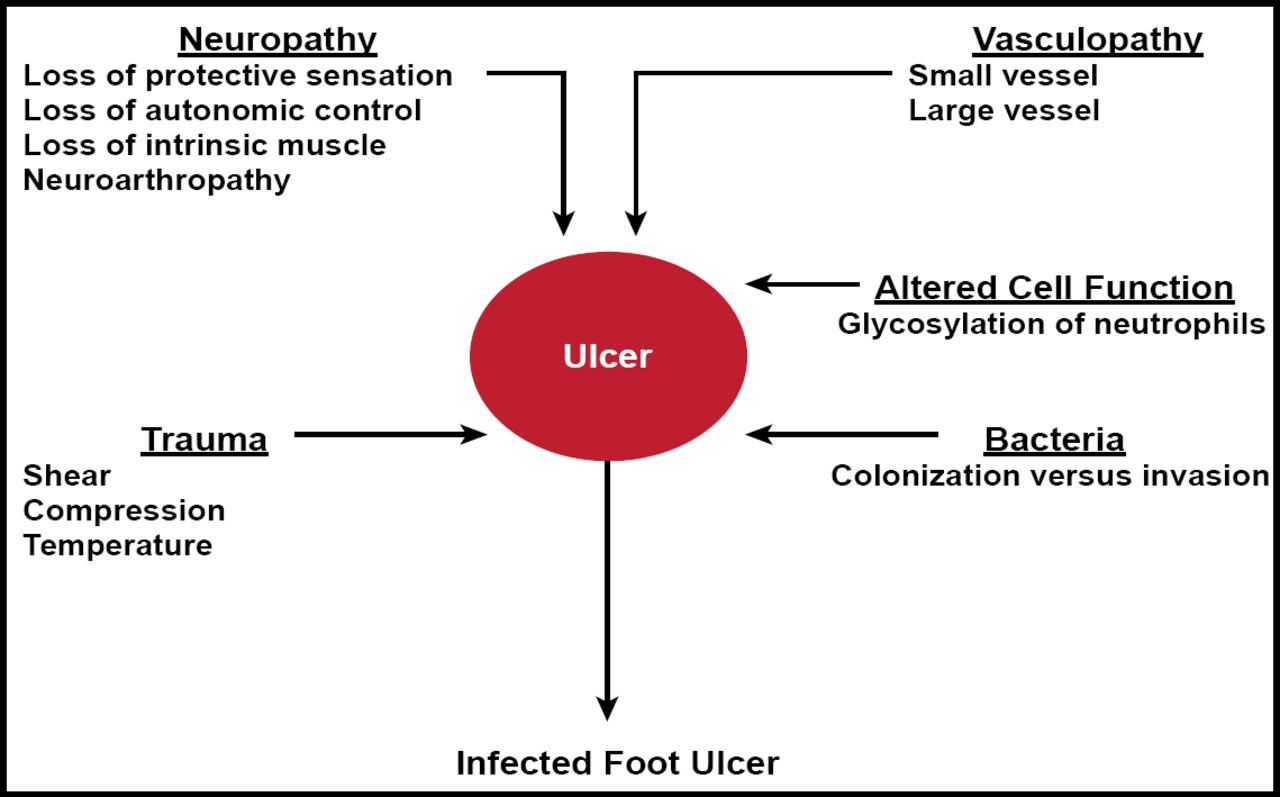
Skin serves many functions. It not only affects sensation and appearance, it also maintains fluid and electrolyte balance, protects the body from microbial invasion, and regulates body temperature. Foot ulcer pathogenesis disrupts these functions (Figure 1). When confronted with an infected diabetic foot, physicians must decide on diagnostic and management approaches, including choice of antibiotic and adjunctive measures.

Foot Ulcer Pathogenesis.
Reproduced with permission from JE Embil, MD.
Diabetic foot infections typically manifest with fever, chills, heat, redness, pus, and pain. Wounds can be colonized but not infected or infected. To manage the wound and infection, physicians must address the underlying cause (eg, neuropathy, unrelieved pressure, repetitive injury, underlying infection, foreign bodies, suboptimal circulation, social factors, and footwear). Dressings and other topical therapies are adjuncts to treatment of the underlying cause.
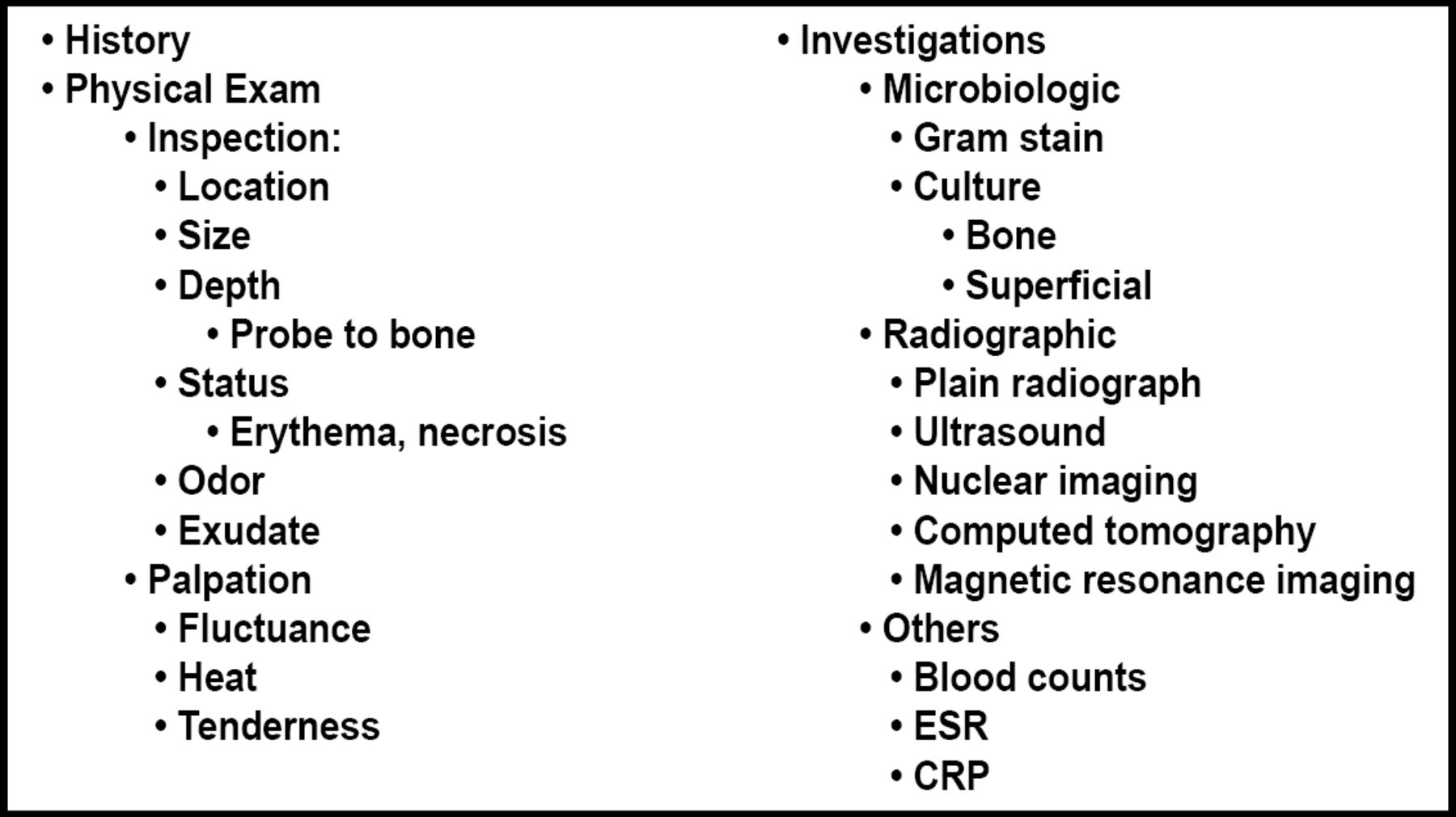
A thorough wound evaluation that includes a history, physical examination, and investigations should guide clinical decision-making (Figure 2). Empiric antimicrobial choices should be broad but based on available microbiology results. The route and duration of therapy will vary, depending on the severity of the infection and the tissues that are involved. Surgical and nonsurgical management of the diabetic foot may be intimately related.

Wound Evaluation.
Therapies for the infected diabetic foot can include oral, parenteral, and topical antibiotics; adjunctive measures; and bed rest with foot elevation. A trial of culture-directed oral antimicrobial therapy may be considered if: 1) the patient and the osteomyelitic lesion are stable; 2) the magnitude of skin, soft tissue, and/or bone involvement is not extensive; 3) therapy can be tolerated; and 4) clinical improvement is ongoing. The alternative is parenteral antibiotics.
The efficacy of adjunctive therapies remains an area of active research efforts. Randomized controlled studies of silver-based or silver-containing topical antimicrobial agents or dressings for treating uncomplicated leg ulcers, acute wounds [Drug Ther Bull 2010], diabetic foot ulcers, or infected or contaminated chronic wounds are sparse, with insufficient evidence for their use in these applications.
Although there is some indication that negative pressure wound therapy may improve healing, clinical evidence is insufficient to prove additional benefit over conventional wound treatment [Gregor S et al. Arch Surg 2008]. Ubbink et al. [Cochrane Database Syst Rev 2008] also found no valid or reliable evidence that topical negative pressure increases chronic wound healing.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.