

Summary
Cardiovascular disease (CVD) is the number one killer of women in westernized countries. Its connection to diabetes, a particularly strong risk factor that disproportionately affects women, has been well established. In a session that was devoted to the implications for CVD prevention and the treatment of women with diabetes. This article discusses differences in current diabetes treatment that are related to gender.
- Prevention & Screening
- Prevention & Screening
- Diabetes Mellitus
Cardiovascular disease (CVD) is the number one killer of women in westernized countries. Its connection to diabetes, a particularly strong risk factor that disproportionately affects women, has been well established. In a session that was devoted to the implications for CVD prevention and the treatment of women with diabetes, L. Kristin Newby, MD, Duke University Medical Center, Durham, North Carolina, USA, discussed differences in current diabetes treatment that are related to gender.
Major randomized controlled trials (RCTs) over the past 1 to 2 decades have changed the practice of CVD prevention in women, with 3 studies having a particular impact on the current guidelines for the prevention of CVD in women. The Women's Health Initiative (WHI) [Rossouw JE et al. JAMA 2002] and the Heart and Estrogen/Progestin Replacement Study [Hulley S et al. JAMA 1998] were, in large part, responsible for the recommendation that hormone therapy not be used for the primary or secondary prevention of CVD, as it is not effective and may be harmful [Mosca L et al. Circulation 2007, 2011]. Aspirin is one of the least expensive and most frequently used preventive therapies for cardiovascular events; however, the Women's Health Study (WHS), which evaluated the use of low-dose aspirin as primary prevention for CVD in women, provided evidence of a sex-based response to aspirin therapy. Among the women in the WHS, aspirin therapy resulted in a significant (p=0.04) overall reduction in stroke (RR, 0.83; 95% CI, 0.69 to 0.99) and a nonsignificant overall 9% reduction in cardiovascular events, a slight increase in the risk of hemorrhagic stroke (RR, 1.24; 95% CI, 0.82 to 1.87; p=NS), and no benefit on myocardial infarction (MI; RR, 1.02; 95% CI, 0.84 to 1.25). To assess for the effect of gender, the authors conducted a gender-specific on aspirin therapy random-effects meta-analysis of data from 6 trials that showed a reduction in risk for MI and no influence on stroke among men but no effect on MI in women and a reduction in the incidence of stroke [Ridker PM et al. N Engl J Med 2005].
Aspirin resistance is present in up to 40% of patients with diabetes, and the prevalence of resistance increases with decreasing metabolic control [McGuire D. Braunwald's Heart Disease: A Textbook Of Cardiovascular Medicine 2012. Elsevier]. Large RCTs are currently evaluating if higher doses of aspirin might overcome the effects of resistance, but the 2011 American Heart Association guidelines state that aspirin (75 mg/day to 325 mg/day) should be used in women with coronary heart disease unless contraindicated and that this therapy is reasonable in women with diabetes unless contraindicated. Signals of an increased risk of MI among younger women and risks for bleeding led to the recommendation against routine use of aspirin in healthy women aged <65 years to prevent MI [Mosca L et al. Circulation 2011].
Finally, although statin therapy greatly lowers cardiovascular risk, in the WHI study, the incidence of new-onset diabetes mellitus was associated with statin use among postmenopausal women [Culver AL et al. Arch Intern Med 2012]. The underpinnings of the recently scrutinized relationship between statin use and new-onset diabetes mellitus are unknown.
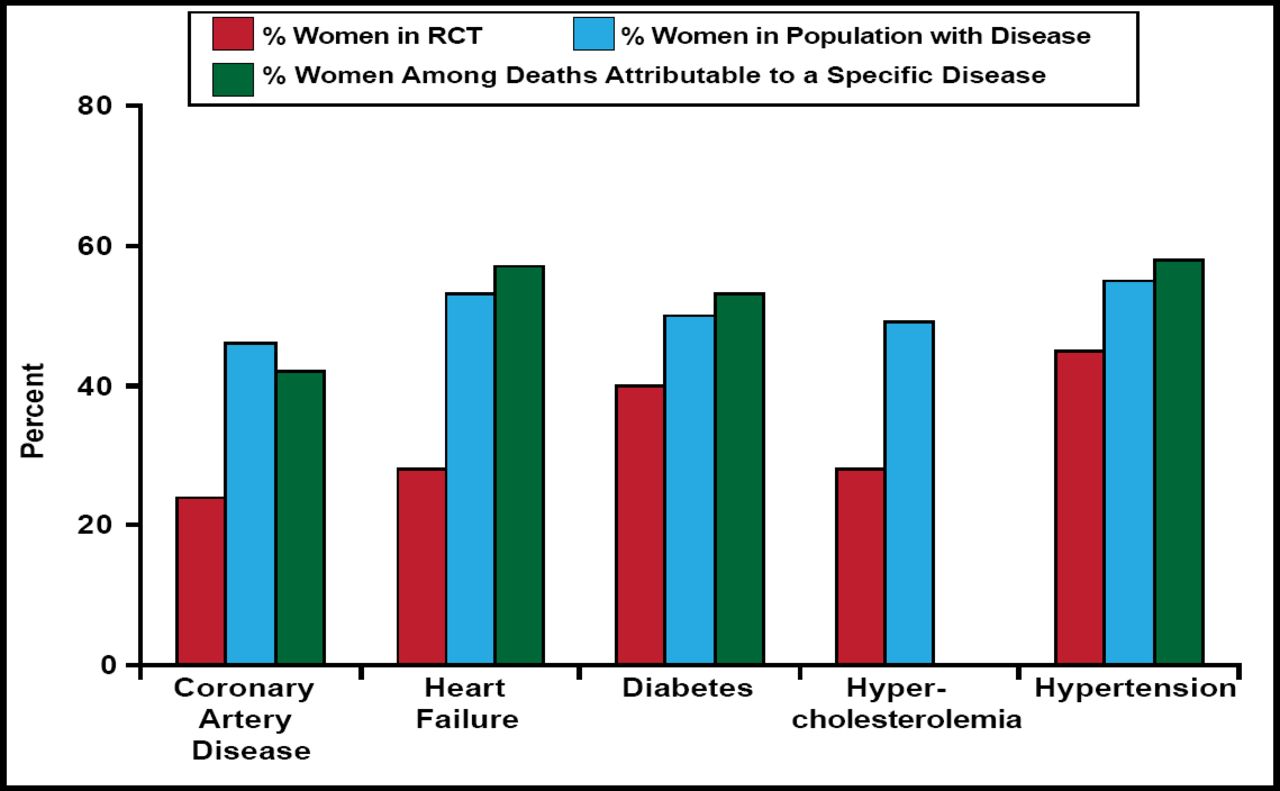
Although the data generally support similar treatment responses in women and men and although there is no clear evidence that diabetes alters treatment benefit of proven therapies in women, the enrollment of women in RCTs remains low, relative to their overall representation in disease populations (Figure 1) [Melloni C et al. Circ Cardiovasc Qual Outcomes 2010]. To ensure that the evidence that supports treatment is relevant to women, more attention must be focused on increasing recruitment of women into randomized clinical trials.

Inclusion of Women in RCTs Supporting Women's Prevention Guidelines.
Reproduced with permission from the American Heart Association. Melloni C et al. Representation of Women in Randomized Clinical Trials of Cardiovascular Disease Prevention. Circ Cardiovasc Qual Outcomes. 2010;3:135–142.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.