

Summary
Hyperglycemia occurs frequently in hospitalized patients and affects outcomes, including mortality, inpatient complications, length of stay, and overall hospital costs [Schmeltz LR, Ferrise C. Hosp Pract (Minneap.) 2012]. This article reviews the latest Endocrine Society Clinical Practice Guidelines for the management of hyperglycemia in hospitalized patients in noncritical care settings [Umpierrez GE et al. J Clin Endocrinol Metab 2012].
- Diabetes Mellitus
- Hyperglycemia/Hypoglycemia
- Nursing
Hyperglycemia occurs frequently in hospitalized patients and affects outcomes, including mortality, inpatient complications, length of stay, and overall hospital costs [Schmeltz LR, Ferrise C. Hosp Pract (Minneap.) 2012]. Observational and randomized controlled studies indicate that improving glycemic control results in lower rates of hospital complications in general medicine and surgery patients [Umpierrez GE et al. J Clin Endocrinol Metab 2012]. Guillermo E. Umpierrez, MD, Emory University School of Medicine, Atlanta, Georgia, USA, reviewed the latest Endocrine Society Clinical Practice Guidelines for the management of hyperglycemia in hospitalized patients in noncritical care settings [Umpierrez GE et al. J Clin Endocrinol Metab 2012].
The guideline objectives include: identifying best practices for recognizing and diagnosing hyperglycemia and diabetes in the hospital setting; identifying appropriate glycemic targets and the rationale for modifying them; understanding how to best reach glycemic targets safely; and recognizing and addressing specific aspects of management (eg, transitions of care and medical nutrition therapy [MNT]).
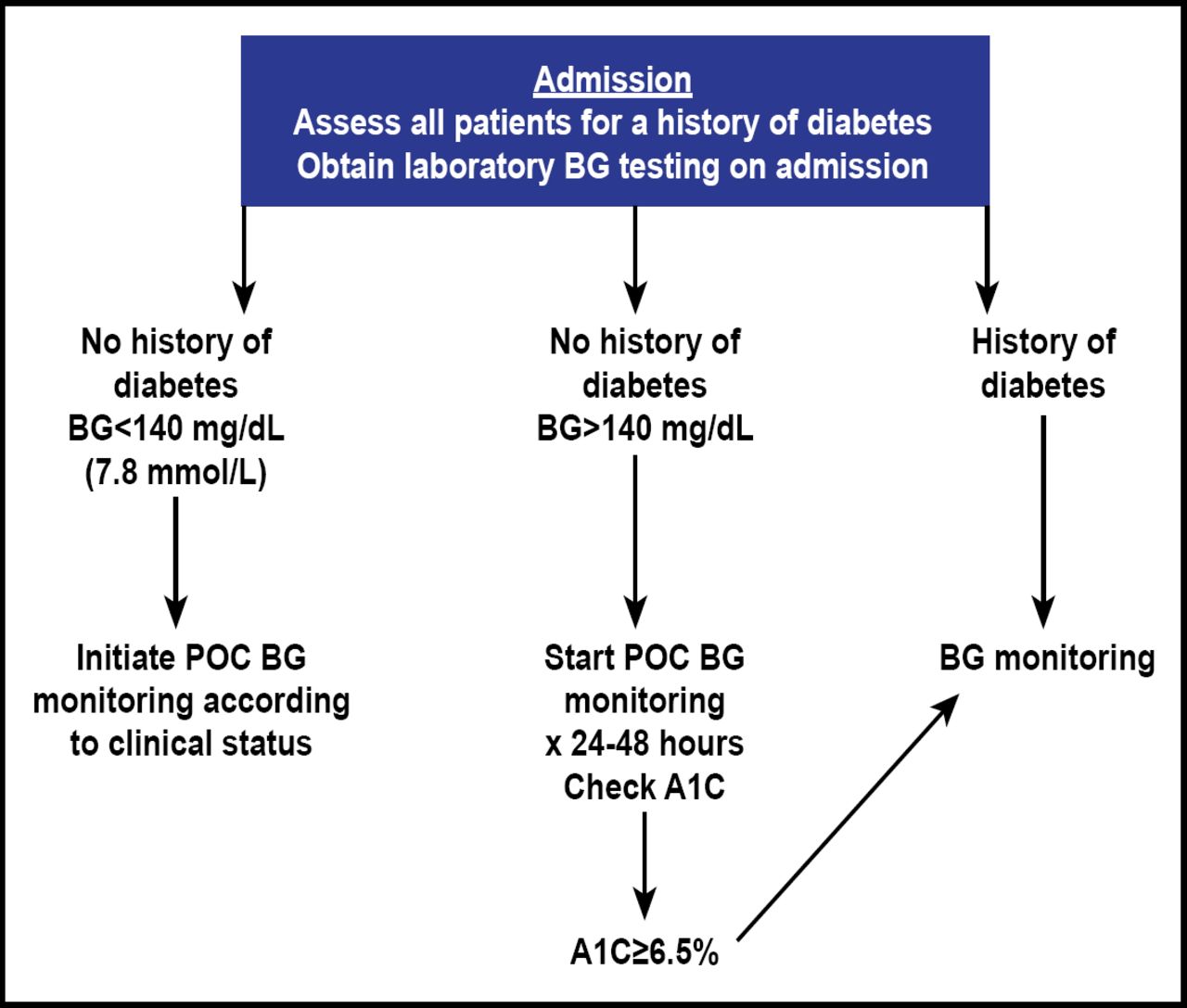
Dr. Umpierrez's presentation covered the diagnosis and recognition of hyperglycemia and diabetes in the hospital setting (Figure 1). He described the benefits and risks of using HbA1C for diagnosis (ie, values can be altered with several conditions, and analysis should be performed using a method that is certified by the National Glycohemoglobin Standardization program) [Suadek CD et al. JAMA 2006].

Diagnosis and Recognition of Hyperglycemia and Diabetes in the Hospital Setting.
Reproduced with permission from G. Umpierrez, MD.
He discussed monitoring of glycemia and glycemic targets (Table 1) in the noncritical care setting (ie, a premeal glucose target of <140 mg/dL [7.8 mmol/L] and a random blood glucose of <180 mg/dL [10.0 mmol/L]) for the majority of patients with noncritical illness [Umpierrez GE et al. J Clin Endocrinol Metab 2012]. He also covered MNT, transition from home to hospital, and pharmacological therapy (eg, scheduled subcutaneous insulin therapy consisting of basal or intermediate-acting insulin given once or twice a day in combination with rapid- or short-acting insulin administered before meals in patients who are eating; Table 2).
Glycemic Targets in the Noncritical Care Setting.
Example of a Basal Bolus Insulin Regimen for the Management of Noncritically Ill Patients with T2DM.
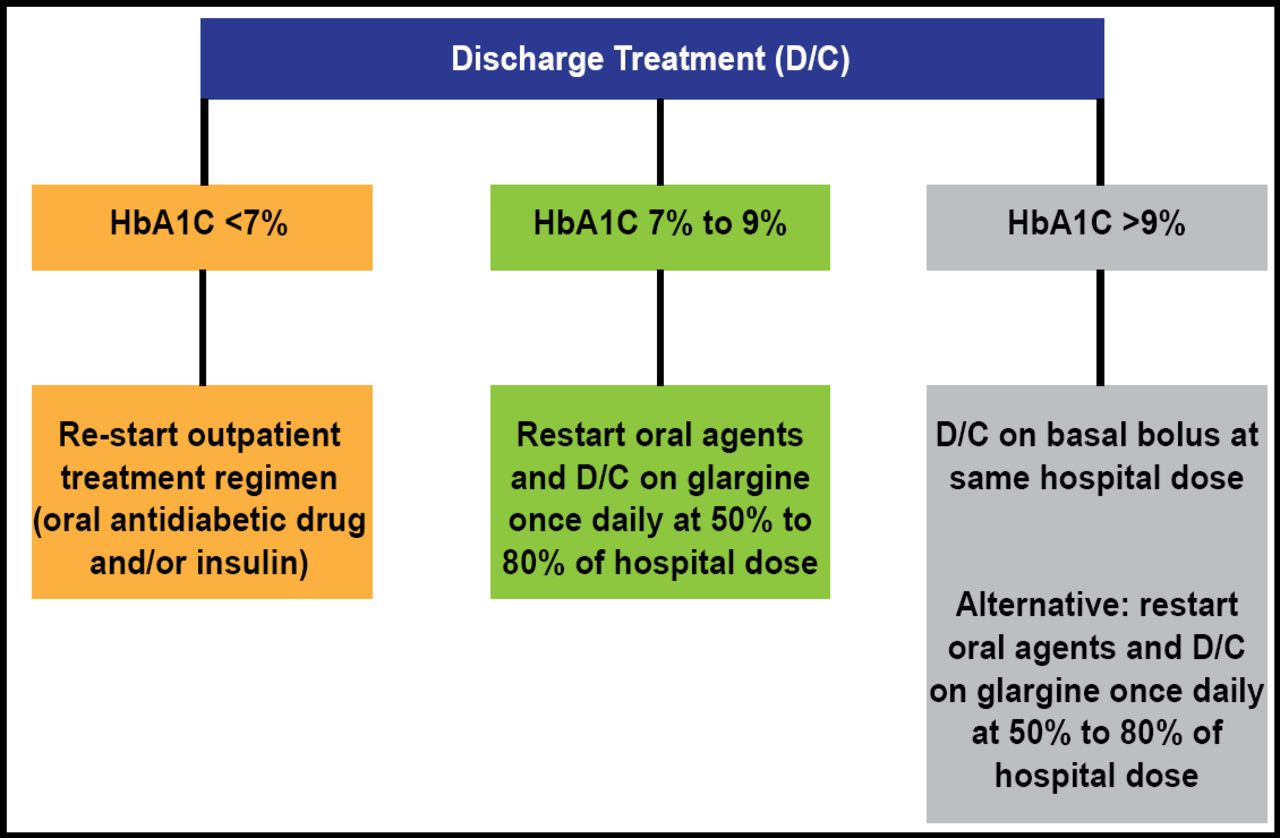
Other topics included pharmacological treatment of hyperglycemia in the non-intensive care unit setting (eg, avoidance of prolonged use of sliding scale insulin therapy as the sole method for glycemic control in hyperglycemic patients with a history of diabetes during hospitalization) [Umpierrez GE et al. J Clin Endocrinol Metab 2012]; insulin therapy in patients with type 2 diabetes [Umpierrez GE et al. Diabetes Care 2007]; and transition from hospital to home (Figure 2).

Discharge Insulin Algorithm.
Reproduced with permission from G Umpierrez, MD.
Special situations include the switch from intravenous continuous insulin infusion to subcutaneous insulin therapy and patients who receive enteral or parenteral nutrition or glucocorticoid therapy. He noted that hyperglycemia during total parenteral nutrition is associated with a greater risk of hospital mortality [Pasquel FJ et al. Diabetes Care 2010].
Dr. Umpierrez stressed that MNT is an essential component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia and that providing meals with a consistent amount of carbohydrates can be useful in coordinating doses of rapid-acting insulin to carbohydrate ingestion. He also reviewed the risks of hypoglycemia in the hospital setting.
According to the guidelines, an in-hospital glycemic control program should include: administrative support for an interdisciplinary steering committee using a systems approach to improve care of inpatients with hyperglycemia and diabetes; a uniform method of collecting and evaluating point-of-care testing and insulin use data as a way of monitoring the safety and efficacy of the glycemic control program; and the provision of accurate devices for glucose measurement at the bedside with ongoing staff competency assessments.
Dr. Umpierrez also specified methods and goals for educating patients and professionals. These include diabetes self-management education that focuses on short-term survival goals; identification of community resources to provide continued support to patients; and ongoing staff education to update diabetes knowledge in general and whenever an adverse event that is related to diabetes management occurs.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.