

Summary
Aquaporin-4 (AQP4) autoantibodies are specific for neuromyelitis optica (NMO) and related spectrum disorders; the specificity exceeds 90%. NMO and multiple sclerosis (MS) share transverse myelitis and optic neuritis as typical symptom complexes, but they tend to be more severe in NMO and often are associated with longitudinally extensive lesions in the corresponding affected central nervous system structures, which are rarely found in MS. While interferon beta and natalizumab benefit MS patients, they appear to exacerbate NMO.
- Demyelinating Diseases
Aquaporin-4 (AQP4) autoantibodies are specific for neuromyelitis optica (NMO) and related spectrum disorders; the specificity exceeds 90%. NMO and multiple sclerosis (MS) share transverse myelitis and optic neuritis as typical symptom complexes, but they tend to be more severe in NMO and often are associated with longitudinally extensive lesions in the corresponding affected central nervous system (CNS) structures, which are rarely found in MS. While interferon beta and natalizumab benefit MS patients, they appear to exacerbate NMO.
Brian Weinshenker, MD, FRCP, Mayo Clinic, Rochester, Minnesota, USA, presented evidence for his argument that MS and NMO are mutually exclusive. AQP4 autoantibodies are highly specific for NMO. However, recently a small number of suspect false positive cases have been detected, typically seropositive with one assay technique, especially Enzyme-linked immunosorbent assay (ELISA), but seronegative with other reference assays, such as tissue and transfected cell immunofluorescence. Dr. Weinshenker cautioned to beware of a positive test result if the clinical story does not fit (ie, the patient does not have longitudinally extensive transverse myelitis, has oligoclonal bands or has brain lesions more typical of MS).
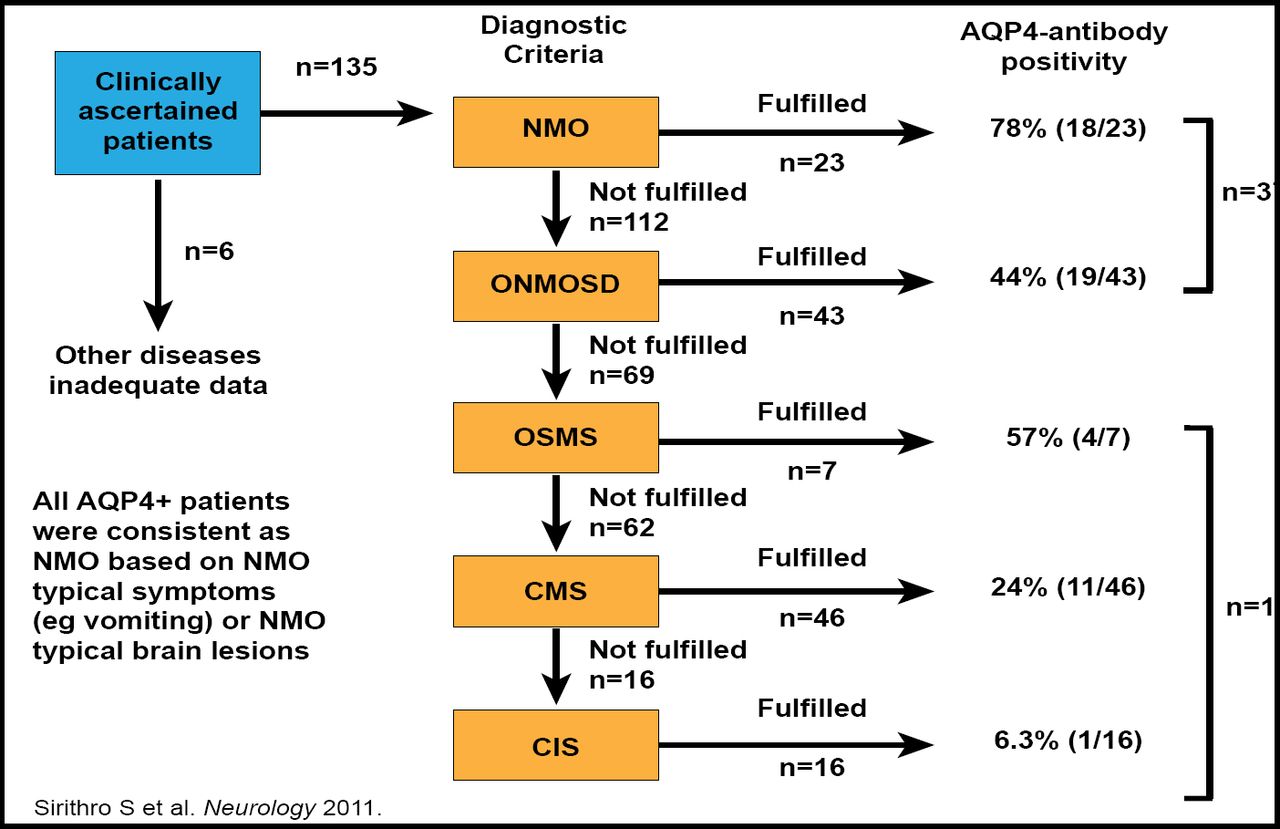
In a Thai study, approximately 16/53 patients who were AQP4+ did not meet the criteria for NMO or NMO spectrum disorder but were diagnosed on clinical grounds as having MS, opticospinal MS (OSMS), or clinically isolated syndrome (CIS; Figure 1) [Siritho S et al. Neurology 2011]. However, in retrospect, these cases were clinically misclassified and clues, such as intractable vomiting or hiccup, were present indicating the patients had NMO.

AQP4 Antibodies “Trump” Clinical Diagnosis in Thai Patients.
Siritho S et al. AQP4 antibody-positive Thai cases: Clinical features and diagnostic problems. Neurology. August 2011; with permission from Lippincott Williams & Wilkins, Inc.
According to Dr. Weinshenker, NMO should not be automatically diagnosed in AQP4+ patients, as false positive results very rarely may occur. However, AQP4 autoantibodies are highly specific, and a positive test should lead to careful consideration of the diagnosis. Physicians should be aware that the spectrum of NMO is broader than previously thought, and some patients clinically diagnosed as having CIS, MS or opticospinal MS may, in fact, have NMO.
Another Perspective
Joab Chapman, MD, PhD, Tel Aviv University, Tel Aviv, Israel, argued that NMO and MS do overlap. He presented a case study of a 15-year-old girl with rapidly progressing paraplegia, who clinically recovered on corticosteroids. Virology, lupus, and other autoimmune workups were negative, including presence of NMO. A clinical diagnosis of MS was made based on neurologic deficits (subacute dissemination in time and space, retrobulbar neuritis, and myelitis), typical MRI lesions, evoked potentials, and oligoclonal bands in cerebrospinal fluid.
NMO disturbs MS dogma because antibody-producing cells and astrocytes (AQP4 is on astrocyte foot plates) play a major role, indicating that the MS complex comprises several diseases of which NMO is the first to be extracted. Prof. Chapman has treated several patients with NMO who also had systemic lupus erythematosus (SLE). This coexistence of autoimmune diseases, especially with SLE, is common, suggesting that NMO may be a manifestation of SLE.
MS also overlaps with antiphospholipid syndrome (APS). Both affect white matter, cause motor disability, cognitive dysfunction, epilepsy, myelitis, are autoimmune disorders, and sometimes have similar magnetic resonance images. The two conditions can be differentiated with electrophysiologic tests; evoked potentials have 78% sensitivity and 90% specificity for differentiating MS from APS. ELISA studies found significantly high (p<0.001) levels of antiphospholipid antibodies in MS patients.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.