

Summary
This article discusses the relative limitations of current commonly used risk predictors for coronary heart disease (CHD) and the results from several studies that used carotid intima-media thickness measurements to improve the prediction of CHD.
- Lipid Disorders
Allen J. Taylor, MD, Georgetown University, Washington, DC, USA, discussed the relative limitations of current commonly used risk predictors for coronary heart disease (CHD) and the results from several studies that used carotid intima-media thickness (CIMT) measurements to improve the prediction of CHD.
“One sees modest accuracy for predicting CHD mortality using the Framingham Risk Score (FRS) and the National Health and Nutrition Examination Survey (NHANES),” Dr. Taylor said. He noted that although the FRS discriminates short-term risk well, it may not identify subjects with low short-term but high lifetime risk for CHD, most likely because of changes in risk factors over time.
The measurement of CIMT may be a useful tool to redefine individual risk of CHD, because increases in CIMT have been shown to be directly associated with an increased risk of myocardial infarction (MI) and stroke in older adults without a history of cardiovascular disease (CVD) [O'Leary DJ et al. N Engl J Med 1999]. A meta-analysis confirmed these results and further established the robustness of the findings across ethnicities and gender. The relative risk of MI was 1.15 (95% CI, 1.12 to 1.17) per 0.10-mm common carotid artery IMT difference [Lorenz MW et al. Circulation 2007]. Adding plaque and CIMT to traditional risk factors improves CHD risk prediction in low- and intermediate-risk groups [Nambi V et al. J Am Coll Cardiol 2010], while adding CIMT as a marker enhances absolute CHD risk discrimination in middle-aged adults with diabetes [Folsom AR et al. Diabetes Care 2003]. A connection between coronary artery calcium (CAC) score and IMT has also been shown. In adults aged >70 years, CAC and common carotid artery (CCA)-IMT had similar hazard ratios for total CVD and CHD. CCA-IMT was more strongly related to stroke than CAC, but CAC was also a predictor of stroke [Newman AB et al. Am J Cardiol 2008].
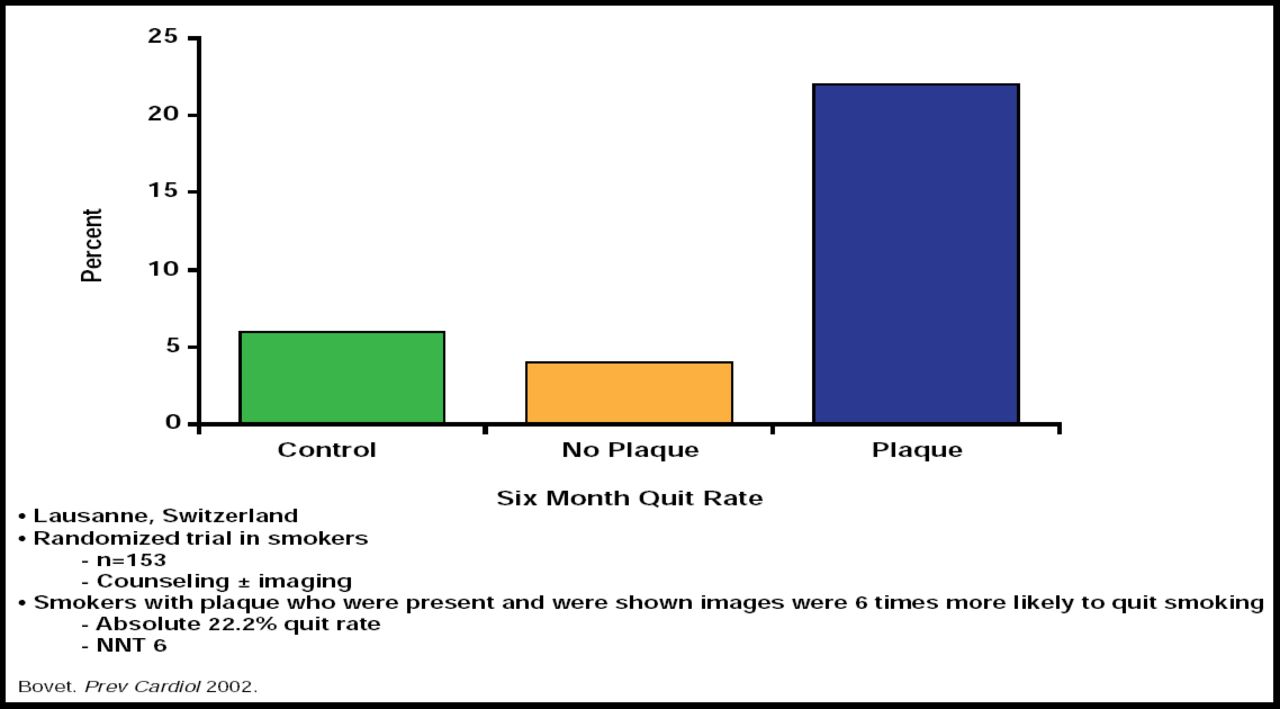
These studies indicate that CIMT is useful in identifying some patients who are at increased risk for CHD, and at least one study suggests it is a good tool for motivating risk reduction. Smokers who were shown CIMT images that revealed the presence of plaque were 6 times more likely to quit smoking (absolute 22.2% quit rate; Figure 1) [Bovet P et al. Prev Med 2002].

Can CIMT Help Motivate Risk Factor Management?
Reproduced with permission from A. Taylor, MD.
The improved prediction rates with CIMT measurement have been encouraging enough for the National Cholesterol Education Program to note it as an option for adjusting risk and therapies in people with multiple risk factors [Grundy SM et al. Circulation 2004]. The Society of Atherosclerosis Imaging and Prevention, in collaboration with the International Atherosclerosis Society, conducted an appropriate use review of common clinical scenarios in which CIMT testing may be considered. Clinical scenarios included the clinical application of CIMT for risk assessment in the absence of known CHD, risk assessment in patients with known CHD, and serial CIMT imaging for monitoring CHD risk status. Appropriate indications were clustered within the detection of CHD risk among intermediate-risk patients, those with metabolic syndrome, and older patients [The Society of Atherosclerosis Imaging And Prevention. Atherosclerosis 2010].
Dr. Taylor concluded by noting the recommendations of the National Cholesterol Education Program and the Society of Atherosclerosis Imaging and Prevention. Specifically, carefully performed measurements of CIMT are appropriate in properly selected patients as a tool to adjust the cardiovascular risk assessment and the therapeutic approach to cardiovascular risk reduction. CIMT is an imaging test and is more resource-intensive than other traditional risk predictors (eg, medical history, blood pressure, LDL-cholesterol). While CIMT may add information to traditional risk predictors, it may only be clinically useful in settings in which findings have the potential to change management; ie, those with abnormal values at baseline. In patients who are known to be high-risk who are already on maximal medical therapy, for example, findings are unlikely to change management. In addition, normal CIMT should be interpreted with caution in patients with other indicators of high risk, such as a high Framingham Risk Score or elevated LDL-cholesterol, as it may underestimate risk. Whether measurement of CIMT becomes integrated into clinical practice remains to be seen, because further prospective controlled studies, including analyses that incorporate costs and compare CIMT with other imaging modalities, are needed.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.