

Summary
For patients with coronary artery disease (CAD), several factors influence the need for revascularization and the optimal revascularization strategy. These include the clinical status of the patient, the extent of ischemia, the complexity of coronary anatomy, and the presence of common comorbidities, such as diabetes.
- Interventional Techniques & Devices
- Diabetes Mellitus
- Coronary Artery Disease
For patients with coronary artery disease (CAD), several factors influence the need for revascularization and the optimal revascularization strategy. These include the clinical status of the patient, the extent of ischemia, the complexity of coronary anatomy, and the presence of common comorbidities, such as diabetes. In this session, presenters discussed changing trends in revascularization for patients with high-risk CAD.
Fractional Flow Reserve: A New Tool for Noninvasive Ischemia Assessment
In weighing the benefits and risks of revascularization, cardiologists must judge whether or not a particular stenosis is likely to cause myocardial ischemia, said Pim A.L. Tonino, MD, PhD, Catharina Hospital, Eindhoven, The Netherlands. In many cases, however, cardiologists do not have sufficient information about the presence or absence of ischemia. Noninvasive testing is an important step for determining if there is a reasonable expectation of benefit with revascularization; yet, the utilization of noninvasive evaluation is poor. In a study of Medicare patients who were undergoing elective percutaneous coronary intervention (PCI), only 44.5% of patients underwent stress testing to document ischemia within 90 days prior to the procedure [Lin GA et al. JAMA 2008].
Even when standard noninvasive studies are performed, these tests are not always accurate in predicting stenosis-related ischemia, particularly in high-risk patient groups, such as those with multivessel disease (MVD). In one recent study, myocardial perfusion imaging with single-photon emission computed tomography underestimated the number of ischemic territories by 36% in patients with MVD and overestimated ischemic territories in another 22% of patients [Melikian N et al. JACC Cardiovasc Interv 2010].
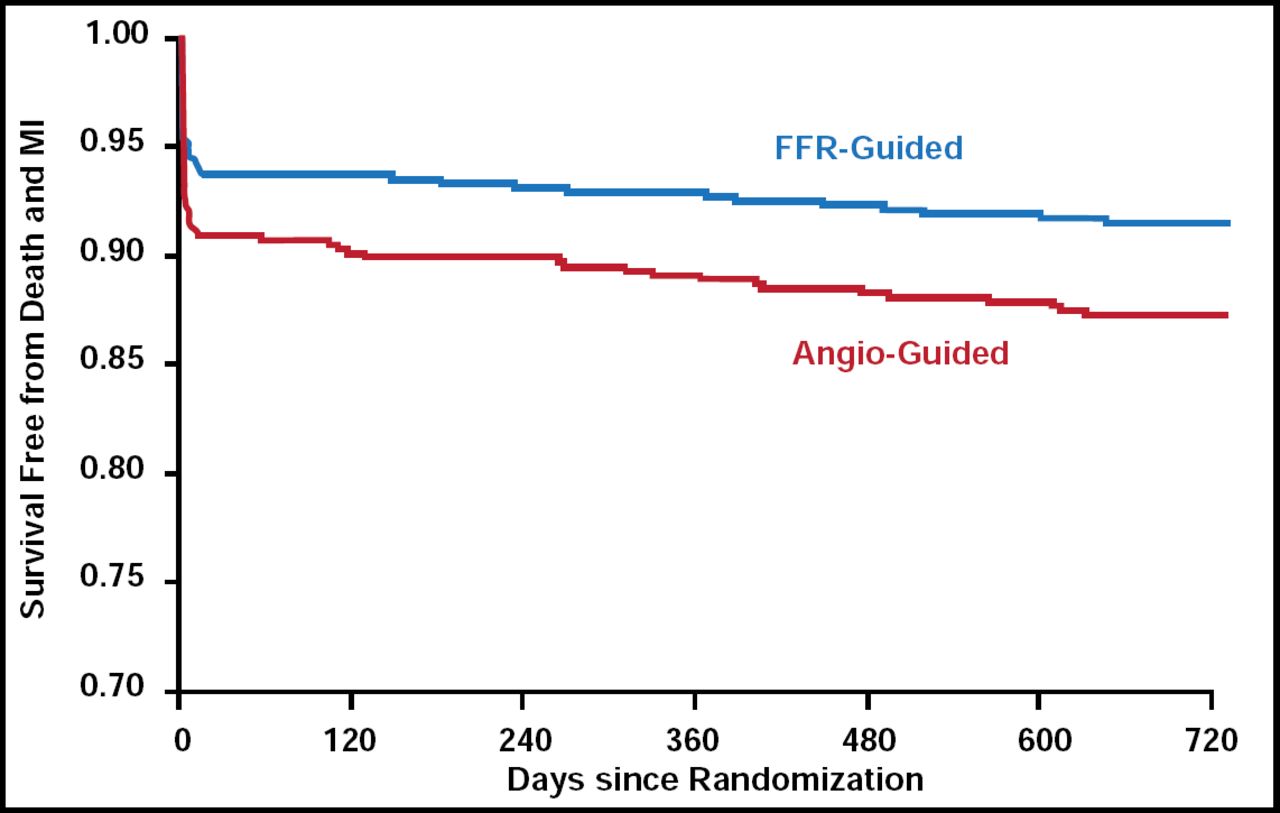
Utilization of fractional flow reserve (FFR) as an adjunct to coronary angiography can improve the accuracy of preprocedure testing. In the recent Fractional Flow Reserve Versus Angiography for Multivessel Evaluation (FAME) trial of 1005 patients with multivessel CAD, routine measurement of FFR improved clinical outcomes and lowered costs compared with standard angiography-guided PCI in patients with MVD. At 2 years, 12.9% of patients in the angiography-guided PCI group and 8.4% of patients in the FFR-guided group met the primary endpoint of mortality or myocardial infarction (MI; p=0.02; Figure 1) [Pijls NH et al. J Am Coll Cardiol 2010].

FAME: 2-Year Freedom from Death or MI with FFR-Guided PCE and Angiography-Guided PCI.
Reproduced from J Am Coll Cardiol, Volume 66, Issue 3, Pijls NH et al. Copyright 2010, with permission from Elsevier.
As an effective tool for assessing stenosis-related ischemia, FFR can improve clinical decision-making about revascularization in patients with MVD, left main stenosis, and other high-risk presentations. Indeed, in the new 2010 European Society of Cardiology guidelines on myocardial revascularization, FFR-guided PCI is now recommended for the detection of ischemia-related lesions when objective evidence of vessel-related ischemia is not available [Wijns W et al. Eur Heart J 2010].
Revascularization: Considerations for Diabetic Patients
Coronary revascularization with coronary artery bypass graft (CABG) surgery is the preferred method of revascularization in diabetic patients with multivessel CAD. However, drug-eluting stents have shown promising preliminary results in the diabetic population, raising new questions about whether the standard of care is changing for this patient population. Valentin Fuster, MD, PhD, Mount Sinai Medical Center, New York, New York, USA, described recent evidence that supports the ongoing use of CABG surgery in patients with diabetes and MVD.
SYNTAX: PCI Versus CABG in Severe CAD
In the Synergy Between PCI With Taxus and Cardiac Surgery (SYNTAX) trial, 1800 patients with previously untreated 3-vessel or left main CAD were randomly assigned to undergo CABG or PCI with drug-eluting stents to determine the better revascularization strategy. Approximately 25% of patients in the SYNTAX trial had diabetes. After 12 months, patients in the PCI group were more likely than those in the CABG group to reach the combined primary endpoint of death from any cause, stroke, MI, or repeat revascularization (17.8% vs 12.4%; p=0.002). Patients in the PCI group were also significantly more likely than those who were treated with CABG to require repeat revascularization within 12 months (13.5% vs 5.9%; p<0.001). Meanwhile, patients who underwent CABG were more likely to suffer a stroke (2.2% vs 0.6%, p=0.003) [Serruys PW et al. N Engl J Med 2009].
In SYNTAX, complex coronary anatomy, as indicated by a high SYNTAX score, increased the risk of suboptimal outcomes only within the subgroup of patients who underwent PCI. In particular, within the PCI group, patients with high SYNTAX scores were more likely to develop major adverse cardiac or cerebrovascular events (23.4%) than those with intermediate (16.7%; p=0.10) or low (13.6%; p=0.71) SYNTAX scores. By comparison, within the CABG group, no association was found between SYNTAX score and risk for adverse outcomes. Therefore, for patients with more complex anatomical features with or without diabetes, CABG appears to be the preferable strategy for revascularization [Serruys PW et al. N Engl J Med 2009].
BARI 2D: Revascularization or Medical Therapy in Diabetes and Stable CAD
The Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial evaluated the role of revascularization versus optimal medical therapy alone in patients with type 2 diabetes. BARI 2D included 2368 patients with type 2 diabetes mellitus and stable ischemic heart disease. Upon study entry, each patient's treating physician determined whether CABG surgery or PCI was the more appropriate choice for revascularization. Patients were then stratified according to CABG or PCI group and randomly assigned to undergo treatment with prompt revascularization and medical therapy or intensive medical therapy alone. After 5 years, survival rates did not differ between the revascularization and medical therapy groups (88.3% vs 87.8%; p=0.97) [Frye RL et al. N Engl J Med 2009].
In the overall BARI 2D study population, a similar proportion of patients remained free from major cardiovascular (CV) events in the revascularization and medical therapy groups (77.2% vs 75.9%; p=0.70). Among patients who were initially identified as CABG candidates, however, those who were assigned to prompt revascularization had significantly fewer major CV events than those who were assigned to medical therapy alone (22.4% vs 30.5%; p=0.01). In contrast, among PCI candidates, the CV events rate was similar, regardless of assignment to the revascularization or medical therapy group (23.0% vs 21.1%; p=0.15) [Frye RL et al. N Engl J Med 2009].
After examining the relationship between the prespecified method of revascularization (ie, CABG or PCI) and study group assignment more closely, the BARI 2D investigators found that the benefit of prompt revascularization was significantly greater for patients who were selected for CABG than for those who were selected for PCI (p=0.002). In particular, among those who were indicated for CABG, the risk of nonfatal MI was lower in the CABG group (7.4%) than in the medical therapy group (14.6%).
Compared with patients in the PCI strata, patients in the CABG strata had more extensive coronary disease, with significantly more 3-vessel disease, proximal disease of the left anterior descending artery, and chronic coronary occlusions. Therefore, the findings of BARI 2D suggest that for these types of patients—with diabetes and MVD or other indications for CABG—prompt revascularization with CABG is preferable to medical therapy alone [Frye RL et al. N Engl J Med 2009].
FREEDOM: Revascularization in Patients With Diabetes and MVD
The ongoing Future Revascularization Evaluation in Patients With Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial will help clarify the optimal approach to revascularization in patients with diabetes [Farkouh ME et al. Am Heart J 2008]. The trial will enroll approximately 2000 patients with diabetes and an indication for PCI or CABG. Patients will be assigned randomly to drug-eluting stents or to CABG with or without cardiopulmonary bypass pump (CBP). All patients will also receive aggressive medical therapy for CAD and diabetes. The primary endpoint is a composite of all-cause mortality, nonfatal MI, or stroke. Patients will be followed for a median follow-up period of 4 years [Farkouh ME et al. Am Heart J 2008].
As the largest trial of its kind to date, the FREEDOM trial should provide definitive data on the relative risks and benefits of PCI and CABG therapy in diabetic patients with a range of baseline clinical and angiographic profiles. Accordingly, the FREEDOM trial promises to provide important guidance for the selection of revascularization strategies for patients with diabetes and multivessel CAD, Dr. Fuster said.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
- Article
- Summary
- Fractional Flow Reserve: A New Tool for Noninvasive Ischemia Assessment
- Revascularization: Considerations for Diabetic Patients
- SYNTAX: PCI Versus CABG in Severe CAD
- BARI 2D: Revascularization or Medical Therapy in Diabetes and Stable CAD
- FREEDOM: Revascularization in Patients With Diabetes and MVD
- Figures & Data
- Info & Metrics
- eLetters
Cited By...
- No citing articles found.